
(The knees experience pressure equal to approximately 3 times the body's weight when walking and approximately 5 times the body's weight when running. In other words, a person who weighs 150lbs puts about 750lbs of pressure on the knee when landing each running stride)
Tears or ruptures of the anterior cruciate ligament (ACL) are a common type of knee injury.
ACL injuries commonly occur in the following instances:
• As a result of cutting, pivoting or single-leg landing, and without any external trauma
•Through a twisting force applied to the knee while the foot is planted on the ground, or upon landing on one foot.
• From a direct trauma to the knee, usually the outside of the knee, as may occur in many contact sports
Injury to the ACL is painful and most individuals report a “pop” in their knee, followed by a feeling of instability that hinders many athletic activities, as well as simple daily activities such as walking down stairs.
Surgery is often recommended to restore knee function, but is not always
Description of an ACL Tear
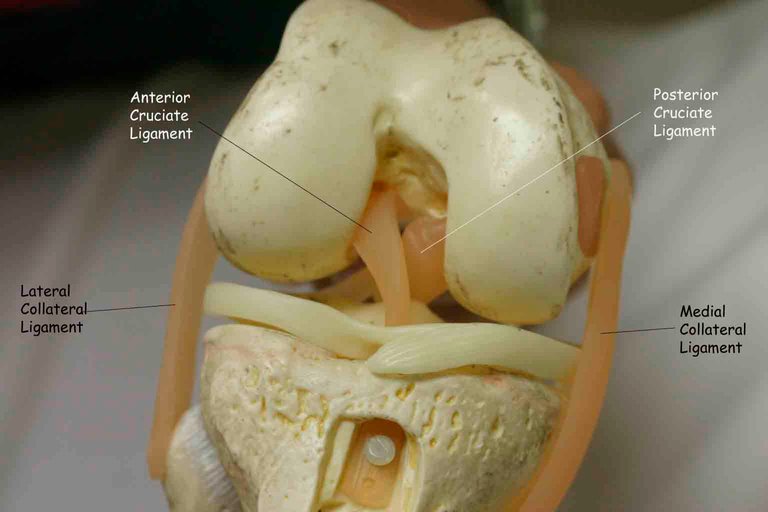
The ACL is one of the main ligaments that help stabilize the knee by preventing the tibia (shin-bone) from sliding forward in relation to the femur (thigh-bone). It attaches to the knee at the bottom back of the femur (thigh bone) and crosses diagonally through the knee joint to attach at the upper part of the tibia (shin bone).
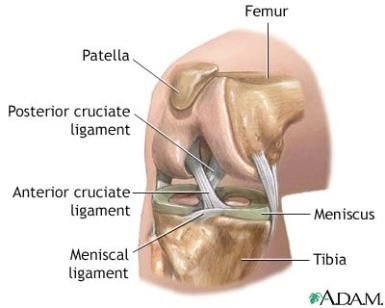
The posterior cruciate ligament crosses the knee joint in the opposite direction, making an X shape (cruciate is from the Latin word for cross). The ACL and PCL work together to provide important stability for the knee joint, especially during movement that involves sudden change of motion or impact.
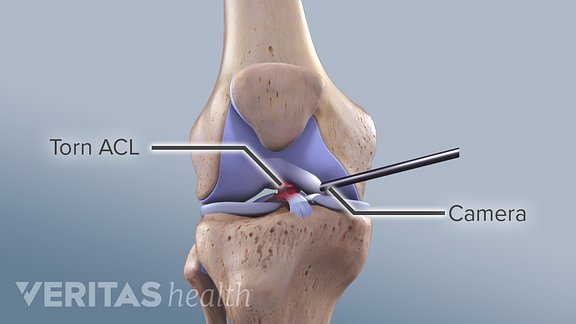
An ACL injury may be diagnosed when the ligament is overstretched or torn. The tear may be partial or complete; a complete tear of the ACL is also known as an ACL rupture.
symptoms

A person who experiences an acute ACL tear often reports some combination of the following knee symptoms:
• Feeling a “pop” at the time of injury
• Immediate swelling after the injury
• Deep pain in the knee
• Instability: the knee feels like it is “giving out”
• Restricted range of motion, with particular difficulty straightening the affected knee
• The knee may feel warm to the touch, due to bleeding within the knee joint
Instability may be especially noticeable during activities that strain the knee joint, such as walking downstairs and pivoting on one leg
Unlike progressive knee conditions, such as knee osteoarthritis, symptoms of an ACL tear are sudden onset and can almost always be traced back to a specific incident or injury.
Without treatment, the swelling and pain in the knee generally subside over a period of several weeks; however the knee instability often persists, limiting the person’s ability to engage in athletics and even daily activities. In particular, it may be difficult for the person to stand up from a sitting position or going downstairs
Additional symptoms
Other structures in the knee, such as (the lateral meniscus 54%) and medical collateral ligament (MCL), are often damaged with ACL injuries. These other injuries may cause additional symptoms, such as knee locking, to occur.
Causes and Risk Factors
While anyone can injure their anterior cruciate ligament, certain factors put people at higher risk:
Cutting, pivoting and single-leg landings.
About 70% of ACL injuries are non-contact injuries that involve sudden deceleration, such as cutting, pivoting or landing on one leg.
They occur most commonly in sports such as basketball, soccer, American football, volleyball, downhill skiing, lacrosse, and tennis.
Video shows mechanism of injury in athete
Female gender. Females are at 4 to 6 times higher risk than males. In fact, year-round female athletes who play soccer or basketball have a rate of ACL-tear of almost 5%.
Previously torn ACL. Once an ACL tear has occurred, the risk of re-tear of the previously repaired ACL is approximately 15% higher than that of the primary ACL tear.
A direct blow to the outside of the leg or knee. ACL injuries from contact typically occur from a direct blow to the knee when it is hyper-extended or bent slightly inward (valgum). For example, an American football player may suffer an ACL tear after an opponent strikes the outside (lateral aspect) of the leg while his foot is planted. An injury that occurs in this fashion may also occur in combination with other knee injuries, such as a medial meniscus tear, medial collateral ligament tear, or cartilage injury.

Age. ACL tears are most common between the ages of 15 and 45, mostly due to the more active lifestyle and higher participation in sports.
Why are women at higher risk for ACL Injuries?

Risk of injury is 2-10x greater than males especially with pivoting sports
ACL injury is more common in females
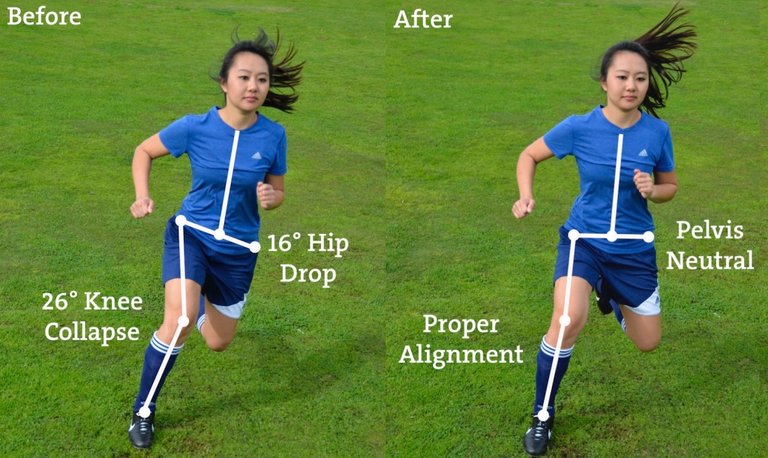
due to landing biomechanics and neuromuscular control differences conditioning and strength play the biggest role females land with their knees in more extension and inward (valgus) due to hip internal rotation , smaller notches , smaller ACL size .
cyclic hormonal levels ACL at greater risk for injury during the first half (preovulatory phase) of the menstrual cycle, leg alignment , some genetic predisposition.
ACL Tear Diagnosis
Physicians and other medical professionals are usually able to make the diagnosis of an ACL tear by the patient's history and physical exam.
Patient interview. A doctor will ask the patient about how the accident or injury happened, symptoms, the pattern of knee pain, and how symptoms affect lifestyle.
Physical exam. A doctor will examine the patient’s knee, noting any swelling, tenderness and pain
A person with an ACL tear will have difficulty bearing weight on the affected leg and the knee will show swelling within the joint. Physical examination tests specifically designed to test the integrity of the ACL are particularly useful when they are also performed on the other (healthy) knee for comparison.
Lachman’s sign is the most accurate ACL injury test. It is performed with the athlete on his or her back with the affected leg relaxed, and the examiner holding the leg with the knee bent at 30 degrees of flexion. With one hand on the thigh for stabilization, a pull forward on the calf will show an increase in motion and soft endpoint compared to the other knee if the ACL is ruptured.
Other tests for the ACL include the pivot-shift and the anterior drawer tests. Caution must be exercised if the examination occurs after significant swelling has occurred because this may reduce their accuracy
Examination of the knee is also performed to evaluate for concomitant injuries to other structures, such as the meniscus and the medial collateral ligament (MCL). These structures can be evaluated by palpating the joint lines and placing the knee through its full range of motion.
For the meniscus, a test called McMurray’s sign is performed by flexing the knee and then internally and externally rotating the tibia while extending the knee.An inward (valgus) force on the knee while it is flexed at 30 degrees may induce pain or laxity if the MCL is injured.Pain upon palpation, or pressing down on, the bony structures around the knee may increase suspicion for a fracture
Medical imaging. A plain X-ray of the knee is imperative if an ACL tear is suspected because of the risk of fracture. An MRI of the knee is utilized to confirm the diagnosis, evaluate for other injuries to the knee, and help plan for surgery.
ACL Injury Treatment Options
Immediately after the injury, management consists of RICE:
rest, ice, compression, and elevation (RICE) of the affected knee.
once an accurate diagnosis has been made then the doctor and patient can move forward with treatment options. Although surgery is sometimes necessary, not everyone who has an ACL injury is a candidate for surgery.
Who should have ACL surgery?

The decision to have ACL surgery depends on many factors, including the patient’s age, activity level, and other injuries.
Age. While there is no age cut-off for surgical intervention, it is rarely performed on individuals over age 55.
Activity level. Surgical reconstruction may also benefit young people and those who participate in occupations or sports that involve jumping, pivoting, cutting, or rapid deceleration.
Associated injuries. Patients with multiple knee injuries (ACL plus meniscus, fracture, or medial collateral ligament) generally benefit from surgery to prevent significant activity restrictions and minimize the already heightened risk of osteoarthritis
While the risk of osteoarthritis is increased after an ACL tear, the effect of surgery on the development of osteoarthritis remains unclear.
Who might not need ACL surgery?

Active individuals who plan to engage in activities or sports that don't involve sudden stops or turns, such as cycling and swimming, and those who do not have knee instability in their daily lives may be candidates for a trial of non-surgical treatment with an experienced physical therapist to maximize strength, balance, and proprioception (body positioning).
Partial ACL tears are usually managed conservatively with a range of motion, strengthening, and addressing proper biomechanics by an experienced physical therapist. Return to sport is generally appropriate once the athlete has achieved strength and motion comparable to the non-injured knee. If instability develops, further evaluation is warranted.
ACL Surgical Repair
Surgery is the most appropriate long-term treatment for some ACL tears. In these cases, the surgeon will remove the torn anterior cruciate ligament and create a new one using a graft.
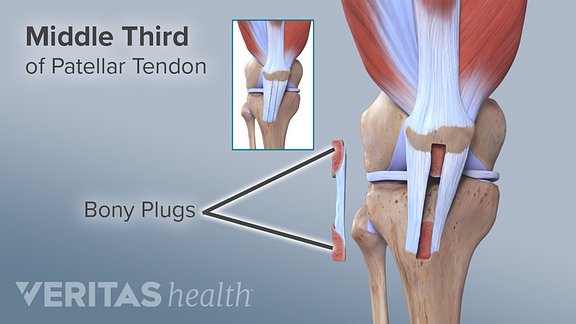
Below are the most common materials used to make an ACL grafts, each with unique benefits.
Patellar tendon. A patellar tendon autograft utilizes the patient’s own tendon to replace the torn ACL, and is beneficial because of its inherent rapid healing.
Hamstring tendon. Autografts using the patient’s hamstring have become increasingly more common because they are not associated with anterior knee pain as in autografts.
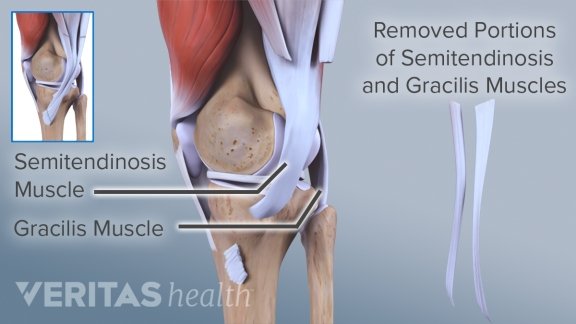
Cadaver tendon. Allografts, which are the utilization of cadaver tendons, are preferred by some surgeons because they do not require removal of the patient’s own tendon.
No specific graft type has proven to be superior aside from that with which a particular surgeon is most experienced.
ACL Surgery Recovery
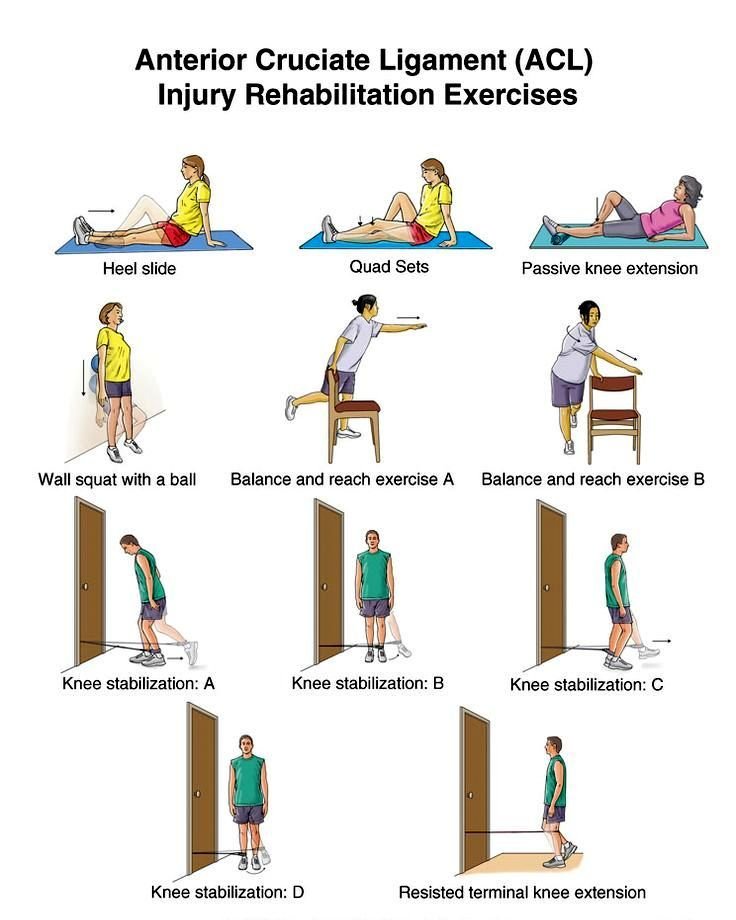
Post-operative rehabilitation is essential to maximize long-term outcomes, emphasizing range of motion, strength, balance, proprioception, and core strength.
While formal physical therapy programs are often recommended, a particularly motivated individual may achieve equally positive results from a home exercise program. Some surgeons recommend the use of knee braces; however there is no evidence demonstrating improved outcomes with their use.
Generally, an athlete can return to his or her sport between 6 and 12 months following surgery.
Only the orthopedic surgeon can determine when it is safe to return to athletic activities.
Returning too soon can put the new ACL graft at risk.
ACL Injury Prevention
Recent attention has focused on prevention of anterior cruciate ligament injuries, especially in young females who participate in high-risk sports.
Successful interventions consist of a multi-component program that include a combination of the following:
• High-intensity jumping plyometric exercises
• Biomechanical analysis with direct feedback to the athlete about proper position and movement patterns, including cutting and landing techniques
• Strength training, especially of the hamstring and gluteus maximus muscles
• Proprioceptive training, such as use of a wobble-board, to improve muscle strength, balance and reaction times
Successful programs have been initiated at least 6 weeks prior to the sports season, followed by an in-season maintenance program that may replace the traditional warm-up.
In addition to changes in training, changes in footwear may decrease the chance of ACL injuries. Shoes with longer or a higher number of cleats seem to increase the risk of ACL injuries.
While some athletes wear knee braces to prevent ACL injuries, current clinical evidence does not support their use.
ACL torn inspiring story
Vanessa Espinoza (female athlete)
you have to be your biggest advocate, regardless of the situation. Maybe you have never played a sport in your life, but some other aspect of your life has been hindered and you are at the point in your life where you have a choice to make.
I went from crutches, to no crutches with a brace, to no brace, to jogging, to agility workouts and finally to playing today. I know that if I would have bowed down at the beginning I would have never seen the field again. Whatever your ACL may be, please do me a favor and kick its ass.
sources
http://www.orthobullets.com

Thank you for reading , upvote and follow
Good article, I have a ruptured lateral meniscus since 1984, my knee used to lock, fortunately it hasn't happened during the last 10 years, cause it hurts like hell to unlock it.
Thank you a lot,, it's good that it resolved hope it never recure again ,, i m here for any consultation
Thank you my freind Muaz great info
Thank you alot freind for support
Wow... A very good educational post.. Learnt something new here today @muazmutasim
thank you very much it's nice to hear that some one learnt from this post , see you again to learn from each other.
Following you!
Congratulations @muazmutasim! You have received a personal award!
Click on the badge to view your Board of Honor.
Do not miss the last post from @steemitboard!
Participate in the SteemitBoard World Cup Contest!
Collect World Cup badges and win free SBD
Support the Gold Sponsors of the contest: @good-karma and @lukestokes
Congratulations @muazmutasim! You received a personal award!
You can view your badges on your Steem Board and compare to others on the Steem Ranking
Vote for @Steemitboard as a witness to get one more award and increased upvotes!