RESULTS AT A GLANCE
Regression analysis reveals average consumption of cereals in Europe between 1993 and 2008 as a significant predictor of schizophrenia burden across 38 countries (R2 = .548, p = < .001). These results triangulate existing literature on carbohydrate consumption, cardiovascular disease, and schizophrenia symptoms, suggesting the presence of common underlying mechanisms that might be uncovered in future research.
INTRODUCTION
Gluten-free and low-carbohydrate diets might help manage symptoms of schizophrenia (1). While case studies and experiments linking these variables are readily found, population studies are lacking. Below, analysis on public datasets (2,3) addresses this gap in the research, reporting on a statistical relationship observed between rates of schizophrenia and consumption of cereals across Europe.
CEREALS AND SCHIZOPHRENIA IN EUROPE
Maps of Europe below define and display values for this study's variables: consumption of cereals (2) and schizophrenia burden (3). Maps are shaded by value in their respective colors. Use the gradient key under each map to find the unit of measurement and scale for values by country.
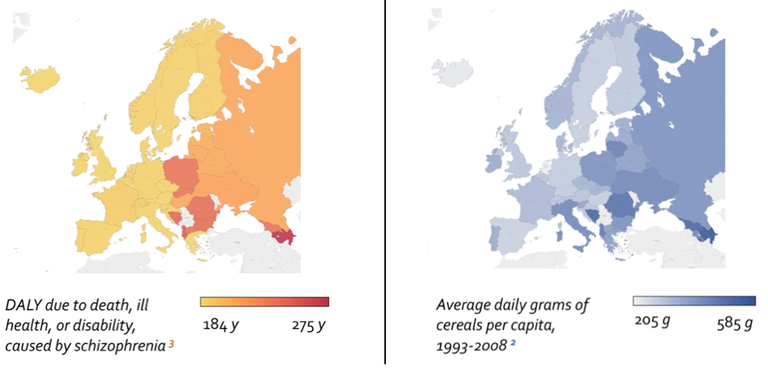
Schizophrenia burden — Europe, 2004.
Schizophrenia burden is estimated by WHO as average years of life lost per 100,000 inhabitants (DALY) due to death, ill health or disability caused by schizophrenia (3). Countries with higher schizophrenia burden are more-red, lower are more-yellow.
Cereal consumption — Europe, 1993-2008.
Darker-shaded countries show higher daily grams of cereals consumed on average (per capita) between the years 1993 and 2008 (2). This variable was calculated by Grasgruber et al (2016) from UN data available at (http://www.fao.org/faostat/en/#data/CC).
The rough similarity in country-shading between the maps above illustrates a link between study variables on a strictly intuitive level. Next, this connection is confirmed through statistical analyses.
STATISTICAL ASSOCIATIONS
Association tests between variables were conclusive, yielding a moderate, but highly significant Kendall’s tau-b correlation coefficient of τb = .442, p = <.001, and a high-moderate R2 value of .548, p = <.001 when predicting schizophrenia burden (3) with cereal consumption (2) (variables as defined above). See scatterplot visualizing the relationship between variables below, where each dot represents a European country’s value per the two study variables.

INTERPRETATION
These results pertain to known relationships between cardiovascular disease, consumption of cereals, and schizophrenia: both schizophrenia diagnoses and cereal consumption are associated with increased risk of cardiovascular disease (2,4), while decreased schizophrenia symptoms have been observed in patients under compliance with a low-carbohydrate/gluten-free diets (1). The present findings triangulate with all this earlier literature, fortifying claims of a positive relationship between carbohydrate consumption and schizophrenia via each of this study’s main variables’ connection to the other (i.e. cereal consumption and schizophrenia symptoms), as well as to cardiovascular disease. Advanced statistical analysis should be deployed to untangle the specific mechanisms underlying all relationships noted.
It's probably not the money. Some will certainly suggest that a central underlying factor in this relationship is differences in wealth across countries. In the bubble chart below, we do see the suggestion of a three-way relationship between Schizophrenia Burden (X axis), cereal consumption (Y axis), and average monthly salary after tax (bubble size, REF. 5).
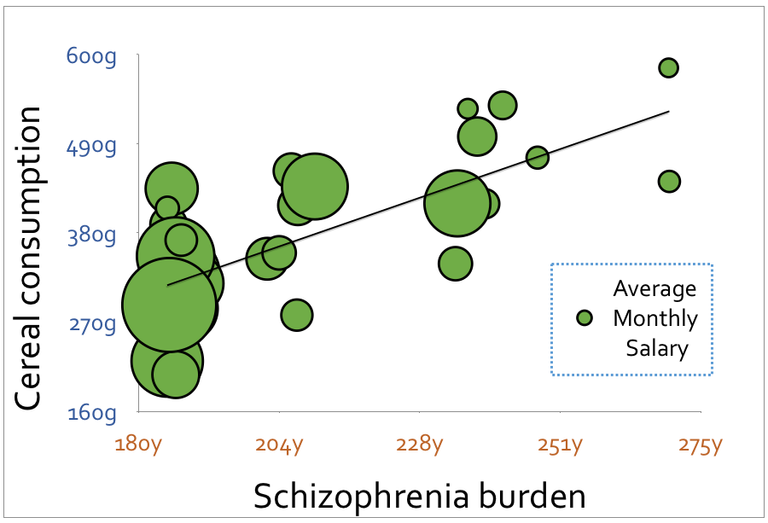
However, this hypothesis does not survive statistical testing. Additional analyses reveal a highly significant linear correlation between schizophrenia and cereal consumption after controlling for salary (r = .560, p = <.001). Further testing is of course needed on the connection between these three factors, preferably using ordinal methods and/or more robust datasets.
REFERENCES.
Kraft, B. D., & Westman, E. C. (2009). Schizophrenia, gluten, and low-carbohydrate, ketogenic diets: a case report and review of the literature. Nutrition & metabolism, 6(1), 10.
Grasgruber, P., Sebera, M., Hrazdira, E., Hrebickova, S., & Cacek, J. (2016). Food consumption and the actual statistics of cardiovascular diseases: an epidemiological comparison of 42 European countries. Food & nutrition research, 60(1), 31694. SUPPLEMENTAL DATA, Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5040825/bin/FNR-60-31694-s001.xlsx. ORIGINAL UN DATA: http://www.fao.org/faostat/en/#data/CC
World Health Organization. (2004). Global Burden of Disease 2004 Update: World Health Organization, 9. Geneva: WHO. DATASET AVAILABLE AT: http://www.who.int/entity/healthinfo/global_burden_disease/gbddeathdalycountryestimates2004.xls
Ringen, P. A., Engh, J. A., Birkenaes, A. B., Dieset, I., & Andreassen, O. A. (2014). Increased mortality in schizophrenia due to cardiovascular disease–a non-systematic review of epidemiology, possible causes, and interventions. Frontiers in psychiatry, 5.
https://www.numbeo.com/cost-of-living/prices_by_country.jsp?displayCurrency=USD&itemId=105
Full plate: