Antibiotic resistant bacteria, A reason for concern?

Introduction
Around WW1, the risk of death due to bacterial infection in flesh wounds was extremely high. 300,000 deaths a year occured from common infections. This all started to change though, after penicillin was commercialised. The rate of finding or inventing new antibiotics started to really ramp up in the 1940´s and did not slow down until after 1980´s and really dropped of after the year of 2000. New regulations and scientific hinders, have made it much less profitable to focus development on antibiotics.[1]
The genetic resistance to antibiotics, is passed between different bacterial species and thanks to high use of antibiotics, resistance has become very common. Bacteria knows how to fight of antibiotics of many kinds, by effluxing, degrading, making it precipitate, aggregate, or bind it to something else, making them harmless. There are for example, 5 known families of efflux pumps that gives the possibility for fast detoxification of the cytosols, all functional against many different molecules. These pumps are much more than antibiotic systems, making it hard to know how antibiotics will work prior to tests.[3] Wild animals never in contact with humanity still carry MRSA due to our water pollutions and sewage waste. Simultaneously, more bacterial species is going resistant due to exposure of other bacteria with resistance or antibiotics in e.g cattle farms. There is already strains like MRSA, that also can pick up the gene vanB, which means it will be vancomycin resistant, a last resort treatment. Even bacteria exposed to chemicals at mining sites, have show diverse immunity against chemicals.[2]
In the case of vancomycin, the bacteria have mutations in many different genes, making it hard to predict or know how this happens, but it results in a slight variation in cell wall structures. Today we see projections of about 10 million deaths a year until 2050 in infectious diseases from resistant strains along with total costs of up to 100 Trillion dollar to battle this developmen.[2] The average rate is less than 4 years after finding a new way to fight the bacteria, until immune strains is found, and it seems to be increasing. This might result in an post antibiotic era which spawned some economical and scientific collaborations the last years aiming to create a larger and more evolving pipeline of antibiotics.[1] In 2015, WHO organized the first Antibiotic awareness week, so they are aware of the issue.
A problem and hopefully a solution with Amdinocillin
Urinary tract infections (UTIs) is when you get an infection in the urinary tract often caused by E. coli which is gram-negative. One in two women get a UTI at least once in their lifetime which make UTIs one of the infections, which require treatment of antibiotic, that is most spread throughout the world. Most UTIs is not life threatening but if the infection spreads into the kidneys and bloodstream, the infection can become very severe. [4] UTIs can develop to Sepsis, which is a life-threatening disease with at least 25 000 cases in Sweden every year and that is more than the three most common forms of cancers, together [5]. Maria Castellucci [6] describes in an article that “Sepsis was present in 6% of hospitalizations from 2009 to 2014. At the same time, sepsis accounted for roughly 15% of in-hospital deaths…”.
Amdinocillin, also known as Mecillinam or Amd, is an antibiotic that have been used for treatment of UTIs since the early 1980s. Amd-treated cells goes from being rod-shaped to enlarged, nondividing spheres that later lyses. Amd causes this change in shape by inhibiting, through binding, the transpeptidase activity of penicillin-binding protein 2 (PBP2) which is responsible for the elongation of rod-shaped cells. [7]
In a study written by Thulin et al. [7] they describes how the resistance against Amd has remained low in clinical studies but in laboratory selections, a large number of resistant mutants have been found. In total, there are 38 genes that can cause Amd resistance when mutated and the expectation is that resistance will become more common in clinical isolations. In the study Thulin et al. observed two crucial differences between the Amdr isolated from clinical setting compared to the laboratory-isolated Amdr were found. The first observed difference was that the range of resistance-causing mutations appeared narrower in the clinical studies compared to the laboratory studies. The other difference was that all the clinical isolates had a mutated cysB gene but only one of the laboratory-isolated mutant had that gene mutated. CysB protein is the dominant positive regulator of cysteine biosynthesis in for example E. coli and the mechanism of how a mutated cysB can lead to resistance is not fully understood. Thulin et al. [7] believes that the resistance is partly due to increased levels of the molecule ppGpp which is responsible for the stress response in reaction to amino-acid starvation amongst others. The presence of ppGpp makes PBP2 nonessential but the mechanism is uncertain.
Thulin et al. [7] investigated the probable causes to why Amd resistance among E. coli remained low in clinical studies and they propose that it is due to two factors. One factor is that most of the laboratory-isolated resistant mutants grow slowly and due to frequent urinating, slow-growing mutants cannot become fixed in the bladder. The other factor is proposed to be that increasing levels of Amd reduces the grow rate and then the recently mentioned problem of stably maintain the bacteria in the bladder occurs.
In another study Thulin et al. [8] investigates the possibility to reverse Amd resistance to susceptibility in E. coli. They discovered that the genetically stable resistance mutation of cysB can be reverted to susceptibility when grown in urine. The believe that the reversion is due to the high levels of cysteine and related thiol compounds. They also found out that the osmolality of urine alters susceptibility; when diluting the urine resulted in increased susceptibility because low osmolality increased early lysis.
The findings that Thulin et al. [8] discovered are important for clinical implications. They suggest that Amd can be used to treat resistant mutants that have been found in laboratory studies and that testing of susceptibility for Amd need to be performed in media that mimics urine. They also show that changes in patient behaviour, for example increased water and cysteine intake, can lead to susceptibility for Amd.
The search for novel antibiotics - Diphenylureas to treat methicillin-resistant Staphylococcus aureus (MRSA)
As for now the majority of all antibiotics are natural products of microorganisms or derivatives thereof called semisynthetic antibiotics. These antibiotics are however starting to become very limited in usability as an increasing amount of bacterial strains are developing mechanisms of resistance. Perhaps the most problematic among these resistant strains are the methicillin-resistant Staphylococcus aureus strains (MRSA). Each year, more than two million people turn ill from multi-resistant bacteria in USA alone. twenty three thousand of these people succumb to the infection and it is estimated that approximately half of these deaths are due to different MRSA strains [9]. This is further complicated by the declining investment in antibiotic research by large pharmaceutical companies.
Fortunately, in 2017, Haroon Mohammad et al reported the discovery of two diphenylurea based compounds with significant effects in the treatment of MRSA.
These two compounds belong to a novel class of antibiotics and they are produced completely synthetically. The compounds are based on the findings of extensive in silico modeling using previously known important antibacterial structures and whole cell assays of a large in-house library of compounds containing said structures [10][11].
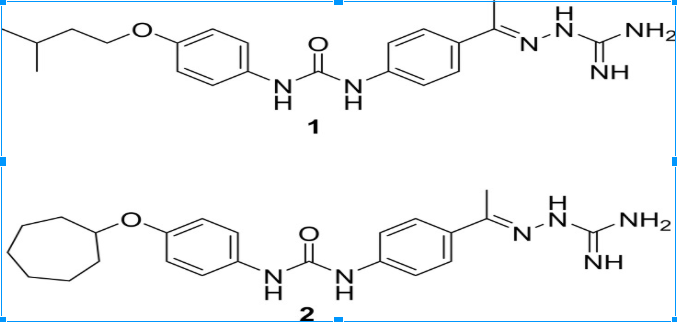
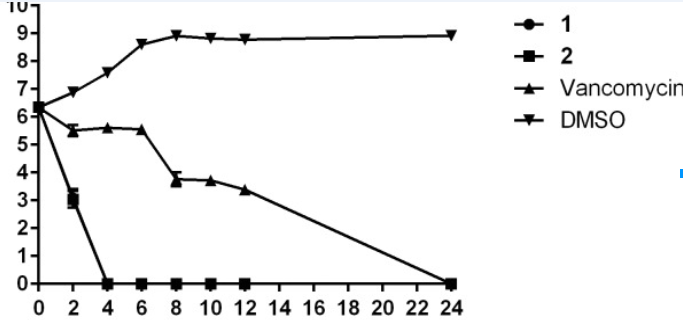
These compounds were presented as lead compounds and exhibited antibiotic effects at concentrations in the ug/mL range. DC-1 inhibited growth of cultured MRSA at 4 ug/mL while DC-2 was effective within the range of 8-16 ug/mL. These values might be considered as a poorer result compared to the minimum inhibitory concentration (MIC) of the so called “last resort antibiotic” vancomycin at 0.5-1 ug/mL. However, the DC-1 and 2 where not only effective against the most common MRSA strains but also against strains that displayed very efficient resistance against mupirocin and vancomycin. To confirm the belief that the compounds are bactericidal a time-kill assay was performed comparing DC-1 and 2 to vancomycin (a confirmed bactericidal agent) and a negative control consisting of dimethyl sulfoxide (DMSO). As can be seen in figure 2, both DC-1 and 2 does in fact display potent bactericidal effects.
The most important discovery was however the MRSA strains inability to display any resistance to these compounds, even after fourteen passages in a multi-step resistance selection assay. The MIC of both DC-1 and 2 remained at a constant level throughout all passages which can be compared to the sevenfold increase in MIC for ciprofloxacin after the fourteenth passage [10].
Synthesis of DC-1 and DC-2
a) Initially, the isocyanate of 4-acetylphenyl isocyanate is reacted with the amine group of 4-aminophenol through a nucleophilic addition to yield 1-(4-acetylphenyl)-3-(4-hydroxyphenyl)urea. The reaction takes place in dry tetrahydrofuran.
b) The hydroxyl group of 1-(4-acetylphenyl)-3-(4-hydroxyphenyl)urea is then alkylated by a suitable allylic or benzylic halide in the presence of dimethylformamide potassium carbonate.
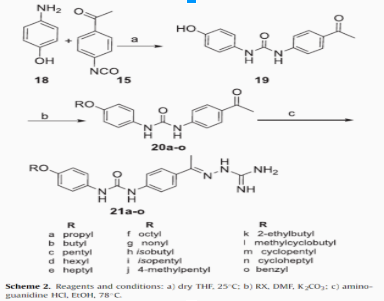
c) Lastly, the acetyl group of the now alkylated diphenylurea analog (20a-o) is reacted with aminoguanidine in the presence of hydrochloric acid producing the final, functional antibiotic through substitution of the carbonyl oxygen [11].
Vancomycin reengineering to overcome resistance: Click Chemistry [1,2,3]-Triazole Vancomycin Dimers
We have the possibility to reengineer the vancomycin molecule by forming 1,2,3 triazole links. This method has shown increased effectivity on VRE(vancomycin resistant enterococcus) & MRSA strains, which is a great addition to the pipeline of antibiotics. This do also allow the usage of existing production capacity and buy time until new compounds is found.
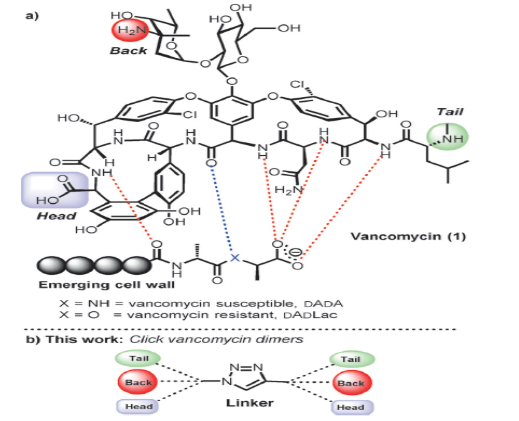
When linking vancomycin into dimers, click chemistry works excellent and vancomycin molecules can be linked at many different positions, to work against VRE or MRSA strains.[5]
The different dimers have different effect on VRE & MRSA strains but many has increased effect. The X molecule in figure 4 dictates immunity, an O-link, gives immunity, but an NH-link don't, due to losing a single hydrogen bond. Designing the dimer to relocate this interaction, increase the mortality rate of VRE & MRSA by multiple factors.
This is a good way of using new insights in biochemistry along with on older molecules to generate needed compounds.
Conclusions:
There are both a problem on the horizon, but also progress towards solutions to halt the death numbers and potential costs, but there are no definite solutions. This situation has spawned many international collaborations and funding programs, showing that we are ready to tackle this issue. There are both novel antibiotics on its way to the pipeline as well as old ones reengineered to be effective against the immune strains that classic vancomycin & methicillin spawned. Click chemistry vancomycin dimers, changed patient behaviour and simulations of antibiotic interaction, are some of the new methods or compounds that address the rise of immune bacteria. We will need more scientific focus on the area to avoid a possible post antibiotic era, due to limited ways to coop with resistance.
Thanks for checking reading, it is much appreciated!

Reference list
[1] Past, Present, and Future of Antibacterial Economics:Increasing Bacterial Resistance, Limited Antibiotic Pipeline, and Societal Implications:
Katherine H. Luepke,1* Katie J. Suda,2 Helen Boucher,3 Rene L. Russo
Pharmacotherapy 2017;37 (1):71–84
[2] Reengineering Antibiotics to Combat Bacterial Resistance: Click Chemistry [1,2,3]-Triazole Vancomycin Dimers with Potent Activity against MRSA and VRE.
Steven M. Silverman,[a] John E. Moses,[a, b] and K. Barry Sharpless
Chem. Eur. J. 2017, 23, 79 – 83
[3] Bacterial multidrug efflux pumps: much more than antibiotic resistance determinants.
Blanco P, Hernando-Amado S, Reales-Calderon JA et al (2016) Microorganisms 4:14
[4] UTIs could soon be life-threatening without new antibiotics. MacKenzie D. 2017-02-27; New Scientist
[5] Sepsis . Linder A et al. 2015; Läkartidningen
[6] Sepsis mortality rate on the rise. Castellucci M. 2017-09-25; Modern Healthcare
[7] Amdinocillin (Mecillinam) Resistance Mutations in Clinical Isolates and Laboratory-Selected Mutants of Escherichia coli. Thulin E, Sundqvist M, Andersson DI. 2015; Antimicrobial Agents and Chemotherapy.
[8] Reversion of High-level Mecillinam Resistance to Susceptibility in Escherichia coli During Growth in Urine. Thulin E, Thulin M, Andersson DI. 2017; EBioMedicine. p. 111-118.
[9] Centers for Disease Control and Prevention. Antibiotic Resistance Threats in the United States, 2013. 2013. p. 1–114
[10] Bacteriological profiling of diphenylureas as a novel class of antibiotics against methicillin-resistant Staphylococcus aureus, Haroon Mohamad et al. 2017.
[11] Diphenylurea derivatives for combating methicillin- and vancomycin-resistant Staphylococcus aureus. Eissa IH, Mohammad H, Qassem OA, Younis W, Abdelghany TM, Elshafeey A, et al. Eur J Med Chem. 2017;130:73–85.
@smartbot tip 1
You will be rewarded 1 SMARTCASH for using this resteem service
ABASINKANGA RESTEEM SERVICE
1 SMART = 0.04 SBD
How To Use SmartCash?
Σ$$$ Tipped @clausewitz
Σ1 SMART! Comment@smartbot helpto claim. Currently the price of SmartCash in the market is$0.115 USDperSMART. Current value of the tip is$0.12 USD. To find out more about SmartCash, please visit https://smartcash.cc.Scary though, to live in a post antibiotic era with no other solutions :P
Nice post!
These long terms give me the heebeejeebees. This is serious stuff those. The ecosystem of bacteria on its own is on another level!!!
Hehe yeah, scary stuff :)
A very good post about medicine. Actually I do not care about medicine. Are you doctor? Thanks for the post.
I am a biochemist if u missed that :) Doctors work on patients not drug development!
I do not like antibiotic medicine, but what you write is my choice.
VRE & MRSA are poor choices :)
You just planted 0.24 tree(s)!
Thanks to @clausewitz
We have planted already 5333.99 trees
out of 1,000,000
Let's save and restore Abongphen Highland Forest
in Cameroonian village Kedjom-Keku!
Plant trees with @treeplanter and get paid for it!
My Steem Power = 25236.47
Thanks a lot!
@martin.mikes coordinator of @kedjom-keku