
Introduction
Today I'm going to talk a little bit about diabetes or to use the correct name diabetes mellitus (DM).
I've previously discussed how I have to take insulin after I developed pancreatitis and on discussing this with others have realised that there is a lot of confusion about what diabetes is and the actual types.
Since I am also a medical doctor I thought it might be useful to cover some of the basics of this common set of conditions.
I will try to make this as short and as easily accessible as possible.
NOTE: This article is for education and informational purposes only. It is not a substitute for medical advice or treatment. If you think you may be diabetic consult your physician.
A little bit of revision on energy metabolism and glucose

Diagram of an insulin molecule.
You probably learned at school that our bodies use 2 main forms of energy:
- Sugars which provide fast or immediate energy
and: - Fats which provide energy more slowly.
The main sugar utilised by the body is glucose.
A certain amount of glucose is required by the body all the time. This requires glucose to be stored.
The storage and blood levels are regulated (mainly) by insulin, a hormone that is produced by the pancreas.
Origins and historical context - what does the name mean?

The following is from an excellent article on the history of diabetes by Dr Ananya Mandal:
Diabetes mellitus is derived from the Greek word diabetes meaning siphon - to pass through and the Latin word mellitus meaning honeyed or sweet. This is because in diabetes excess sugar is found in blood as well as the urine. It was known in the 17th century as the “pissing evil”.
The term diabetes was probably coined by Apollonius of Memphis around 250 BC. Diabetes is first recorded in English, in the form diabete, in a medical text written around 1425. It was in 1675 that Thomas Willis added the word “'mellitus'” to the word diabetes. This was because of the sweet taste of the urine.
NB: There is also a condition called diabetes insipidus. This has some similar symptoms to DM but has a completely different cause which is not related to energy metabolism. The wikipedia article gives a good summary and I will link it in the references in case you want to find out about it.
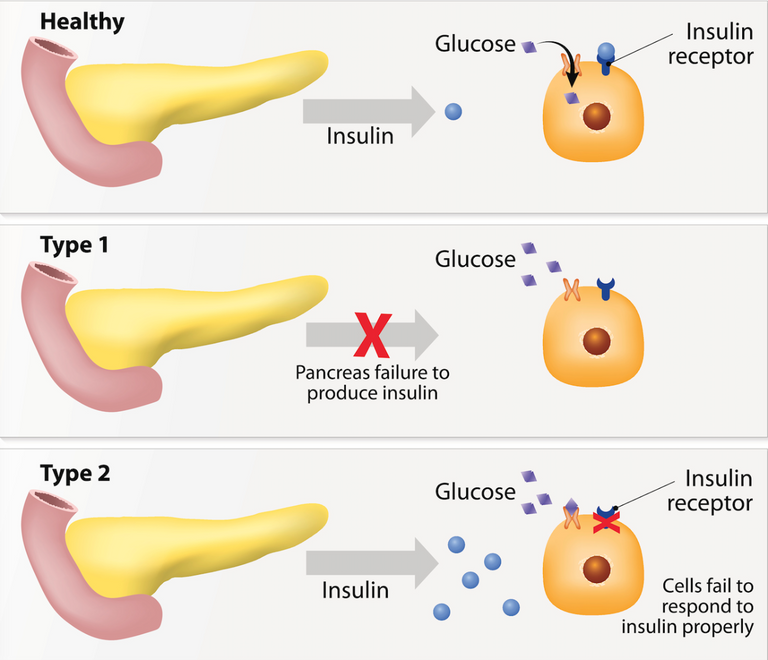
The 2 Types of Diabetes Mellitus
The central feature of diabetes is a either a lack of insulin, or a reduced sensitivity to insulin.
In the former case (lack of insulin) we refer to it as type I diabetes.
In the latter case (reduced insulin sensitivity) we refer to it as type II diabetes.
It is probably more complicated than this but for the purposes of this article we don't need to get into that.
The end result of reduced insulin or insulin sensitivity is an elevated blood glucose level known as hyperglycaemia.
Why is elevated glucose bad?
Glucose is actually quite a reactive compound. It undergoes various reactions with cellular components which cause damage.
One of the most serious ways that this affects health is by causing damage to blood vessels (particularly small ones).
This is the main cause of the complications of uncontrolled diabetes.
Type 1 DM - Summary of Features:

- Usually adolescent onset but can occur at any age.
- Main cause is destruction of the pancreatic cells which produce insulin - commonly due to an autoimmune response (although there are other causes which are beyond the scope of this article).
- Patients must have insulin.
- Patients are prone to weight loss and ketoacidosis if inadequately treated.
- 30% concordance in identical twins (meaning the likelihood of both twins having it), this suggests a primarily environmental component e.g. cross reactivity with certain viruses.
NB - ketoacidosis is a complication that occurs when the body is mainly metabolising fats, you may be familiar with the term ketosis. In certain diabetic patients this can run out of control causing an excess of ketones that can be life threatening. You can read a simple explanation here.
Type 2 DM - Summary of Features:

- Used to be called Non Insulin Dependent DM or NIDDM. Changed since sometimes these patients require insulin.
- This is the type that is rising and we hear about most in the news.
- Associated with lifestyle factors: obesity, lack of exercise, alcohol excess, older age.
- Strong genetic influence - greater than 80% concordance in identical twins, also higher rates in men, Asian origin.
Symptoms for both types

These are mostly due to elevated blood glucose or hyperglycaemia which is the medical term (low blood glucose/hypoglycaemia will be considered separately):
- Increased frequency of passing urine (your kidneys can't work correctly when your blood glucose goes above a certain level).
- Increased thirst - this is mainly due to increased water loss due to point 2 so you dehydrate more quickly.
- Unexplained weight loss - this is because it becomes harder for your tissues to utilise glucose (lack of storage) and so your body starts breaking down fats and muscle tissue both as alternative energy sources and to create new glucose (gluconeogenesis). Remember your body ALWAYS needs a certain amount of glucose.
- Tiredness/Lethargy - a general lack of energy during daily activities.
- Visual disturbances (blurred vision).
- Infections such as thrush (candidiasis) indicating impaired blood supply and immune function.
- Loss of or Altered Sensation - due to nerve damage.
Diagnosis

This is usually via tests done by your doctor:
- In the UK a fasting blood level of >7 mmol/L of glucose is normally used.
- There is also something called an oral glucose tolerance test which can be used. (The patient is given some glucose and their blood levels are tested after 2 hours).
- HBA1C is another test that is frequently done - this gives an estimate of long term glucose control. It is an indicator of glucose reacting with the haemoglobin in your blood. Above 48mmol/L or 6.5% is considered abnormal.
Treatment for Type 1 DM

For type 1 diabetes it is pretty simple - insulin. Insulin cannot be absorbed orally and must be administered as a subcutaneous injection.
There are different types (long, intermediate, short acting) which can be combined in different ways.
A common method is as follows and is the method I use. There are other regimens too though and the type you use will be determined by discussion with your diabetic team:
- Long acting insulin once per day.
- Short acting insulin before every meal.
- Regular testing of blood glucose (finger prick method) prior to meals and also more frequently under certain circumstances (e.g. hypoglycaemia, when driving, alterations to diet/exercise etc.).
Treatment for Type 2 DM

This is dependent on severity:
- Initially education and lifestyle advice : diet, exercise etc.
- Control other cardiovascular risk factors: BP, smoking, cholesterol.
- Medication: Some of these can cause hypoglycaemia (like insulin). It is beyond the scope of this article to go through them in detail.
- Insulin may be required in some cases.
Both types need regular review:

- This can be done in a diabetic clinic either at a hospital or in the community at your GP or Health Centre.
- In the UK these are normally multidisciplinary with a diabetologist/physician, diabetic nurse and dietician.
- Blood tests will be done regularly to check levels of glucose, HBA1C, liver and kidney function.
- It is also common to test things like cholesterol, blood pressure, triglyceride (blood fats) due to the associated risk factors for cardiovascular disease.
- There also needs to be regular testing of general physical health, eyes, feet and extremities to look out for vascular complications.
What is hypoglaecemia?
This is basically "low blood glucose" and usually results from having too much insulin or anti-diabetic medication for the circumstances.
Not all anti-diabetic medications cause hypoglycaemia - for example it is almost unheard of in patients taking metformin alone. The greatest risk is from insulin.
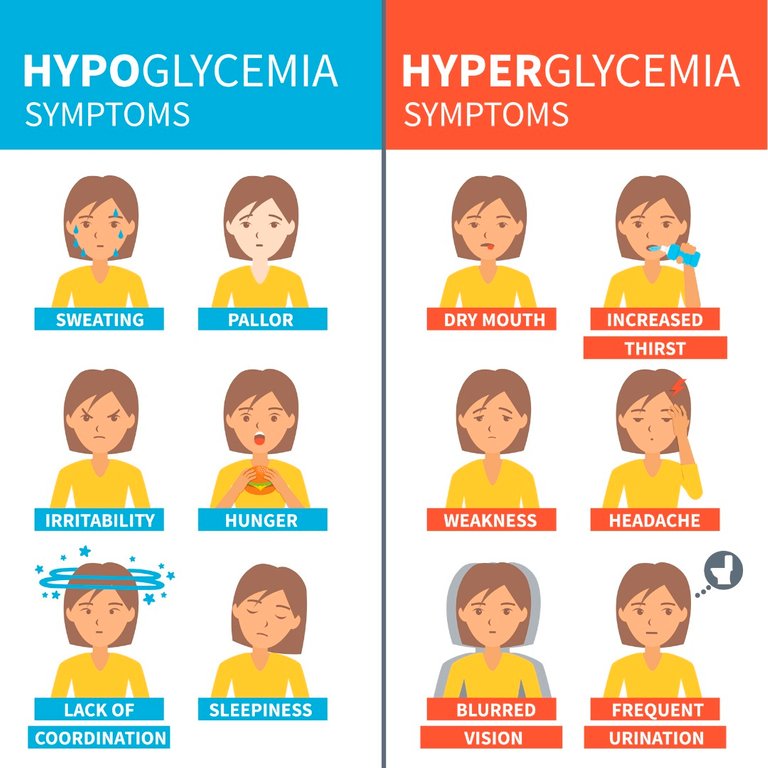
Symptoms include:
- Shakiness
- Nervousness or anxiety
- Sweating, chills and clamminess
- Irritability or impatience
- Confusion, including delirium
- Rapid/fast heartbeat
- Lightheadedness or dizziness
- Hunger and nausea
- Sleepiness
- Blurred/impaired vision
- Tingling or numbness in the lips or tongue
- Headaches
- Weakness or fatigue
- Anger, stubbornness, or sadness
- Lack of coordination
- Nightmares or crying out during sleep
- Seizures
- Unconsciousness
As I stated before you need a certain amount of glucose all of the time (particularly for the brain). If it falls too low that can result in loss of consciousness and ultimately death.
Why does hypoglycaemia occur?

It usually occurs when you have either overestimated how much insulin you need or for some reason you have not eaten as much as you expected - e.g. nausea, vomiting during illness. Exercise can also sometimes catch you out.
Certain types of exercise can reduce your insulin requirement (e.g. aerobics, walking). Other types particularly weight training (in my personal experience) increase the amount you need (probably due to release of stress hormones).
Treating hypoglycaemia

The treatment for hypoglycaemia is to eat something sugary - this can be either something that contains glucose or regular sugar (sucrose which is part glucose).
I usually carry some glucose tablets with me (they taste horrible) but they have been useful on several occasions.
After taking about 15-20 grams of glucose you need to check it again after 15 minutes. It is also recommended to have a small snack (usually something starchy) afterwards to maintain glucose levels until your next meal (if it is more than an hour away).
My experience of hypoglycaemia
For me it manifests in two different ways depending on how quickly my blood glucose falls.
- If it happens slowly I tend to become very irritable and argumentative. I can also get a throbbing headache.
- If it falls more quickly I get a severe panicky sort of feeling, with sweating, a racing pulse and dizziness.
Complications of inadequately treated diabetes

As I stated before inadequately treated diabetes causes damage to all the tissues and organs in your body. The greatest toll is taken on small blood vessels. The main complications are:
- Cardiovascular Disease - e.g. angina, heart attacks and stroke.
- Nerve Damage (neuropathy) - this can cause tingling, numbness, loss of sensation, insensitivity to pain, erectile dysfunction.
- Kidney Damage (nephropathy) - this can lead to kidney failure which may require dialysis or transplant.
- Eye Damage (retinopathy) - this is due to damage and extra growth of blood vessels in the eye. Due to the way the vertebrate eye works new vessel growth is bad. Blindness can be the end result. There is also increased risk of cataracts and glaucoma.
- Foot Damage - due to both loss of sensation and vascular impariment. Wounds to the foot are less likely to be noticed and healing is impaired.
- Skin Conditions - e.g. bacterial and fungal infections due to vascular impairment and reduced immune access.
- Hearing Impairment - this is more common in diabetes.
- Dementias e.g. Alzheimer's disease - poor control of blood glucose is associated with this although the exact mechanism is unknown. Also note the association with stroke mentioned previously also increases the risk of associated vascular dementia.
NB - This is not an exhaustive list and we are learning more all the time.
Conclusion

I hope this has given a useful summary of diabetes mellitus without being too long and you have found it easy to understand.
Since I also have type 1 diabetes myself I think it gives me a unique perspective that other health professionals often don't have. Feel free to ask me any questions :)
Please let me know what you think and also let me know of any errors so I can correct them!
Thank you for reading.

Sources:
J. Murray Longmore, Murray Longmore, Ian Wilkinson. 2014. Oxford Handbook of Clinical Medicine. 9th Edition. Vol. 1. Oxford University Press.
Cashin-Garbutt, April. 2009. “History of Diabetes.” News-Medical.net. December 3. http://www.news-medical.net/health/History-of-Diabetes.aspx.
“Hypoglycemia (Low Blood Glucose).” 2017. American Diabetes Association. Accessed January 3 2017. http://www.diabetes.org/living-with-diabetes/treatment-and-care/blood-glucose-control/hypoglycemia-low-blood.html?referrer=https://www.google.co.uk/.
“Diabetes Complications - Mayo Clinic.” 2017. Mayo Clinic. Accessed January 3 2017. http://www.mayoclinic.org/diseases-conditions/diabetes/basics/complications/con-20033091.
“Diabetes Mellitus.” Wikipedia, The Free Encyclopedia. Accessed: January 3 2017. https://en.wikipedia.org/w/index.php?title=Diabetes_mellitus&oldid=758143915.
“Diabetes Insipidus.” Wikipedia, The Free Encyclopedia. Accessed: January 3 2017. https://en.wikipedia.org/w/index.php?title=Diabetes_insipidus&oldid=749177916.
If you like my work please follow me and check out my blog - @thecryptofiend
All uncredited photos are taken from my personal Thinkstock Photography account. More information can be provided on request.
Are you new to Steemit and Looking for Answers? - Try https://www.steemithelp.net.
Fantastic article, efficient and clear summary. You have inspired me to share my diabetes II experience and how I got it under control.
Thank you that is excellent.
Wow, thank you so very much for one of the very best, if not the best, article I have read on Steemit.com!!! You get my upvote and a total re-steem as well. Awesome work and followed from here on as well. Namaste :)
Thank you:)
This post has been ranked within the top 10 most undervalued posts in the second half of Jan 03. We estimate that this post is undervalued by $24.89 as compared to a scenario in which every voter had an equal say.
See the full rankings and details in The Daily Tribune: Jan 03 - Part II. You can also read about some of our methodology, data analysis and technical details in our initial post.
If you are the author and would prefer not to receive these comments, simply reply "Stop" to this comment.
Thank you:)
I've read some articles that say reversal of type 1 and 2 is possible with calorie restriction and carb reduction. What do you think of this?
For type 1 no because no matter what you do you need insulin and it is potentially dangerous if someone is suggesting that. The best you can hope for in type 1 is that you might reduce your insulin requirements by reducing your sugar intake.
For type 2 you can certainly reduce the severity with lifestyle changes as in most cases of type 2 they are producing enough insulin and the problem is due to reduced sensitivity. This can be altered by diet and exercise.
An amazing article @thecryptofiend
Very informative without being too complicated. I've always gotten the two types of Diabetes mixed. My mother-in-law suffers with type II mainly due to her lack of good diet and exercise. Weight has been a serious issue for her - which also stems from a negative mindset (IMHO).
Thanks so much!
Thank you...very informative! I got more out of your article than from many doctors I've consulted. I have Type 2 and use Metformin and Lantus although I've pretty much been able to stop the insulin injections because of dietary modifications. Another good resource, particularly for people that don't have it yet, is a book by William Dufty called Sugar Blues...I recommend everyone should read it. Thanks again.
Thanks glad you found it useful!
This is very interesting. My gf's grandmother has this pretty severely... thank you for shedding some light on a truly terrible disease.
You're welcome. Yes I think particularly with type 2 most people don't realise how serious it can be!
Post was very helpful. I am grateful to my paintings you see on the page.
outrageous post m8 ! i had a smiliar idea on my mind as well
Thank you. You should do it - this is by no means comprehensive. I had to cut a lot out to make it readable:)
i belive you
Thank you for this information. You did big effort for it. How much time did you take to make this post?
A lot of hours I've been working on it for a while:) The hard part is actually cutting it down to make it simple and easy to understand - thank you for your kind words.
Great Information
Thank you:)
What do you think of the work of Dr. Fung who claims intermittent fasting can cure insulin resistance (type 2 diabetes)?
I would need to see some research to really comment properly. It is certainly likely that it would help. Fasting is good for us for a whole host of reasons.
I am not diabetic myself but this is a stunning article which will be an abundance of help to people who are
Thank you for your kind words:)
Wow, @thecryptofiend.
What an unbelievably useful article about a condition that affects so many. My aunt has diabetes so your write-up can also be used as a great reference guide for me to learn a lot more.
Thank you, @thecryptofiend. It stuns me every time I see a post by you how knowledgeable and structured you are. :)
Thanks so much. You are too kind:)
Wow, great work with this post Arif. Really well organized, lots of information about diabetes. Plus your collection of photos really shows its value in posts like this, where you are able to so effectively complement the information. I really like the sugar skull and crossbones.
Bummer that you have type 1 diabetes though.
Thanks so much. Yes the type 1 sucks. Hoping for a stem cell cure.
I read something about that not too long ago. IIRC there have been some promising breakthroughs in that area as of late. Though it still may be far off....
Yes I had a friend who was working on preliminary research on using haemopoietic stem cells extracted from patient's own blood that were being reprogrammed to differentiate into beta-islet pancreatic cells that produce insulin.
That was the ultimate aim of the research but it was not anywhere near human testing stages.
The early results in animals were very promising. Simply injecting the cells back into the animals after modifying them completely restored insulin function (in the animal models of type 1 diabetes).
This was a few years back but as you know medical research has to go through a long process!
With these sort of treatments (using stem cells in particular) I think the main worry and risk is of cancers - particularly since they are your own cells that have been restored to a near embryonic state.
If something goes wrong there is no easy way to switch them off or eliminate them.
Some sort of master kill switch would be very useful in case of those kind of emergencies.
Further in cases where the original cause is autoimmune some kind of immunosuppression may be necessary in order to prevent the new cells being destroyed and that increases the cancer risk further.
Luckily for me the cause was probably not autoimmune as I had pancreatitis so basically my pancreas digested itself - so I might not need it but in the majority of cases autoimmunity seems to be at least partly responsible.
I'm sure it is only a matter of time though before we get these kind of treatments.
It's tough to get all of the cells to revert to the same correct state or so I was reading. Engineering in a genetic kill switch to the cells might be a good Idea, but that has its own set of ethical concerns attached to it. People are anxious enough about these being in food, I can only imagine the uproar that would occur if it was being done with human cells... being used to treat patients.
Yeah, I truly hope we get stem cell treatments going, all of the literature I have read has been showing basically miraculous recoveries in animal models.
Yes for sure there are lots of problems! I don't remember the specific details of how they were getting around the issue of the correct differentiation state. One way of doing it (though incredibly work and cost intensive) would be to just filter out the types of cells you need but that would not be efficient.
The kill switch thing would definitely be a problem ethically. What if someone used it in a healthy person that wasn't having problems?
It is inevitable because of the potential money to be made. I am sure they will solve the major problems. The big question is when.
@thecryptofiend your posts are always intelligently written yet comprehensive.
So doc, I mean @thecryptofiend.. is there a certain diabetes type where a person gets overweight and they just work out , reduce weight , change their diet and in a few weeks they're free from insulin? I've seen a tv series of such in here and it's amazing. Unfortunately, it seem to just work on obese ones.
In type 2 diabetes you can reduce the severity with diet and exercise but it is rare to completely get rid of it. The only thing that can cure it is gastric bypass surgery - it is still not understood why.
@thecryptofiend A few years back, I remember having this discussion with Dr Day, an endocrinologist who has done some ground breaking research and whom I believe to be the author of the study you're thinking about.
What I recall most was the discussion on options because I was looking at prediabetes myself.
He explained that the reason bariatric surgery is effective at all is the restriction in food uptake, which results in a reduction of fat and the reduction in fat decreases insulin resistance.
The loss of weight from gastric bypass is literally a starvation effect. But for type 2 diabetics gastric bypass is ill advised due to slower wound healing times. However lapbands which are far less invasive, have been used with good success on morbidly obese patients who are also type 2 diabetic. I wish I had a citation, I'm going from memory here.
A lot of heavy fat makes you insulin resistant. Remove the fat, and you remove the insulin resistance. Ergo eat a solid diet and get plenty of exercise, but if you're looking at heart failure each time you exercise, then a lapband can be used to get your weight down low enough you can move around without having a heart attack.
The other advantage to lapbands besides being less invasive is that they can be adjusted and even removed if necessary.
Dr Day's website
https://intermountainhealthcare.org/locations/utah-valley-hospital/medical-services/diabetes-care/diabetes-resources/
More info on lapbands...
https://en.wikipedia.org/wiki/Adjustable_gastric_band
That's what I thought too but it has been refuted by studies.
The normalisation of blood glucose has been noted to occur as soon as 48-72 hours post surgery and at most within a week. This goes against the previous belief that it was a weight loss effect.
I don't currently have Athens access to see the full article but this paper from the July 2013 issue of Science suggests a possible mechanism:
http://science.sciencemag.org/content/341/6144/406
One further mechanism that I have heard suggested is the alteration of gut microbiota:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3652229/
That's interesting. Thanks for the follow up. I hadn't looked at this since 2008 or so. So you have any info on the refutation studies? I work at a hospital and am in a position to let people who are making these recommendations know about the info.
Perhaps refuted is a bit strong of a word for me to use! I think there is growing evidence that it is related to other factors than overall weight loss but that probably contributes too.
It's hard because I don't have academic access to journals right now as you know most of them are behind expensive paywalls! I think the best people to ask would be your endocrinologist colleagues - they can do a Medline search or if the hospital has a good library with a librarian they can do it for them to look for the latest reviews.
The other good source of information is bariatric surgeons they tend to be up to date with the latest research - that is how I found out about this information myself initially and I've read various supporting articles on Medscape etc.
Further in discussions I have had with my own endocrinologist who works directly as part of the bariatric team he is definitely of the opinion that weight loss is not the main cause of resolution. I might ask him for more information at my next appointment.
Actually I just found this article which suggests there may still be some controversy over it although it is from 2013:
http://care.diabetesjournals.org/content/36/Supplement_2/S287
Here is one from Nature Reviews but it is behind a paywall and the abstract doesn't really say much:
http://www.nature.com/nrendo/journal/v9/n10/full/nrendo.2013.159.html
I see, thanks doc @thecryptofiend. One of my friends have it, she's 65 and skinny and going on a diet won't work. She does move a lot and walk much so she actually has not much of a problem with it - just that she's always hungry and thirsty :)
Is she seeing a doctor about it? It sounds like she has poor control and the symptoms you are describing are consistent with high blood glucose levels. The fact that she is skinny may indicate that she may have type 1 or a mix of the two - I would suggest she gets a full assessment from an edocrinologist/diabetic specialist.
@thecryptofiend yes, she always has a blood sugar check up or something like that .
I think if she is still having symptoms like you describe she needs more intensive treatment.
Very cool
Thanks:)
This is a topic that I follow closely and have studied for almost 20 years. Thanks for raising the attention level and educating. Information and treatments for both types mentioned (as well as what may be newly identified types) is always changing and it's important to keep the base facts in mind.
Thanks yes. I'm hoping that it won't be long until our own stem cells can be used to regenerate a damaged pancreas so I can stop taking insulin:)
Very impressive the post. It seems to me that the information we all must know. A bit late my response. But thanks for sharing @thecryptofiend. Greetings. :)
Glad it was useful!
I found it very practical. :)
My grandfather, he suffers from diabetes, and your guide seems very complete. ;)
Great:)
Thanks.
Hi @thecryptofiend, how are you?
I wanted to ask you, if I can try to translate your post into Spanish, and publish it?
I would put that it is of your property, so that it is not seen as plagiarism. I think it is a very good information to share.
I wait your answer. Greetings. ;)
Sure feel free.
Thank you very much. ;)
Did you even read what I wrote because to me it sounds like you didn't?
Great I've never met you before in my life and yet you seem to be acting like you know me. Prevention is always better than treating after development of disease but this kind of argument does not help people who already have problems.
Further how would this attitude help people like me who need to take insulin?
It is clear you are aggrieved about something but that is not my problem.
You clearly have no idea what you are talking about. I'll just leave it at that.