The mortality statistics for COVID 19 have been incessantly hammered into our heads by the mainstream media (MSM). Every day they report these hardest of facts to justify the lockdown (house arrest) and to prove to us that living in abject fear of the COVID 19 syndrome is the only sensible reaction. Apparently, only the most lucrative vaccine ever devised can possibly save us.
The COVID 19 mortality statistics are the reason millions will undoubtedly download contact tracing (State surveillance) apps. This will help the vaccinated to secure their very own immunity passports (identity papers) and enable them to prove they are allowed to exist in the post COVID 19 society, whenever the State demands to see their authorisation.
But how reliable are these statistics? What do they really tell us about what is happening outside the confines of our incarceration? Do they reveal the harsh reality of an unprecedented deadly virus sweeping the nation or does the story of how they have been manipulated, inflated, fudged and exploited tell us something else?
The Once Reliable Office Of National Statistics
In order to register a death in England and Wales, under normal circumstances, a qualified doctor needs to record the cause of death on the Medical Certificate of Cause of Death (MCCD). They must then notify the Medical Examiner for a corroborating opinion. Providing the doctor is clear on the cause of death and no irregularities or suspicions are noted, if the Medical Examiner concurs, there is no need to refer the death to a coroner.
The second opinion of the Medical Examiner (another qualified doctor) was introduced in 2016 following a series of high profile systemic abuses. The mass murderer Dr Harold Shipman, and doctors at Mid Staffordshire NHS Foundation Trust and Southern Health NHS Trust, covered up crimes and widespread malpractice by improperly completing MCCD's.
Today, once the Medical Examiner agrees, they then discusses the death with a qualified informant. This is usually someone who knows the deceased. It is an opportunity, more often than not, for a family member or friend to discuss any concerns about the suggested cause of death. If no further issues are raised, the death certificate can be issued to the informant, the Local Registrar notified and the death recorded.
Registered deaths have been recorded in England and Wales since 1837. From 1911 onward the cause of death has been coded in accordance with the International Classification of Diseases (ICD). Maintaining registration records was the responsibility of the General Register Office until 1970 when it became a department of the Office of Population Censuses and Surveys (OPCS). In 1996 the OPCS merged with the Central Statistical Office (CSO) to form the Office of National Statistics (ONS).
There have been some tweaks and legislative changes to the system over the years. Technology has sped things up a bit, but essentially the simple process of recording registered deaths has changed little over the last century. The ONS have been accurately recording registered deaths in England and Wales for more than 23 years.
From a statistical perspective this consistent, verifiable system has allowed meaningful analysis to inform public health practice and policy for decades. The inbuilt safeguards, maintained and improved over the years, means the ONS provide some of the most reliable mortality statistics in the world.
They record all registered deaths no matter where they occurred in England and Wales. Whether the deceased died in hospital, a care home or in the community, once registration is complete the ONS add it to their statistics.
For weekly statistics the ONS week runs from Saturday to Friday and the statistics are released 11 days after the week ending date. There may be an additional lag for a small number of more complex cases. However, all are eventually resolved and the ONS record the registration of the death in the week it was notified. The ONS also release mortality statistics on a monthly, quarterly and annual basis for comparison.
This does not suit a hungry MSM eager to sensationalise reported COVID 19 deaths. Nor does it serve the immediate interests of State officials who want the public to accept their own house arrest.
Consequently the MSM have reported COVID 19 mortality statistics from a variety of sources. Some from the NHS, some from the Department of Health and Social Care (DHSC) and eventually the ONS. Now the Care Quality Commission have also been thrown into the mix.
Ultimately, all of these deaths will be registered. The ONS will record them and it will be possible to know how many died, the causes of death and the trends identified.
Except in the case of COVID 19.
The Vague Case Of A COVID 19 Death
The Coronavirus Act 2020 received Royal assent on March 25th. This had significant implications for the registration of deaths and the accuracy of ONS data in relation to COVID 19.
Not only did the act indemnify all NHS doctors against any claims of negligence during the lockdown, it also removed the need for a jury led inquest. Effectively, only in the case of death from the notifiable disease of COVID 19. Worrying as these elements of the legislation are, they are just part of a raft of changes singling out registered COVID 19 deaths as unusually imprecise.

The NHS issued guidance to assist doctors to comply with the new legislation. Any doctor can sign the MCCD. There is no need for the scrutiny of a second Medical Examiner. The Medical Examiner, or any other doctor, can sign the MCCD alone. The safeguards introduced in 2016 were removed, but only in the case of COVID 19.
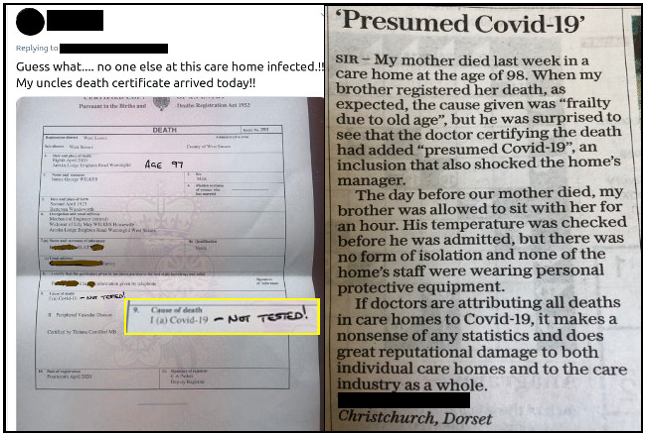
Doctors do not necessarily need to have examined the deceased prior to signing the MCCD. If it is considered impractical for the doctor who last saw the deceased to complete the MCCD, providing they report that the deceased probably had COVID 19, any other qualified doctor can sign the death certificate as a COVID 19 death.
There is no requirement for any signing doctor to have even seen the deceased prior to issuing the MCCD. A video link consultation within the 4 week period leading up to the patient's death, is deemed sufficient for them to pronounce death from COVID 19.
If that were not tenuous enough, as longs as the signing doctor believes the death was from COVID 19, potentially absent any examination at all, perhaps simply by reviewing the patients case notes, if a coroner agrees, a COVID 19 death can still be registered.
The coroner's agreement is practically a fait accomplis. On the 26th March the UK State released guidance from the Chief Coroner. This was intended as advice to all coroners in cases of COVID 19 referral.
There were some notable changes to normal coronal procedures. Paragraph 5 strongly reminded coroners of their obligation to maintain judicial conduct. It stated:
"The Chief Coroner cannot envisage a situation in the current pandemic where a coroner should be engaging in interviews with the media or making any public statements to the press."
This thinly veiled threat to coroners made it clear that speaking out about any concerns would be considered a breech of judicial conduct. A career ending act it would seem.
The NHS guidance advised that if no signing doctor has seen the deceased prior to registration of death, a referral to the coroner must be made. This is a procedural recommendation not a legal requirement. A legal requirement is only applicable in cases of unknown or suspicious causes of death. In turn, the Chief Coroner's guidance states:
"COVID-19 is a naturally occurring disease and therefore is capable of being a natural cause of death......The aim of the system should be that every death from COVID-19 which does not in law require referral to the coroner should be dealt with via the MCCD process."
The Coronavirus Act 2020 also meant that a qualified informant, who agrees the cause of death on the MCCD, no longer needed to be anyone acquainted with the deceased. A hospital official, someone who is ‘in charge of a body’ or a funeral director can perform this vital function. The Chief Coroner advised:
"For registration: where next of kin/informant are following self-isolation procedures, the arrangement for relatives (etc) should be for an alternative informant who has not been in contact with the patient to collect the MCCD and deliver to the registrar for registration purposes. The provisions in the Coronavirus Act will enable this to be done electronically as directed by the Registrar General."
Most relatives, or someone acquainted with the deceased, will be following self isolation procedures. They will almost certainly be terrified of contracting COVID 19 because they have just been told their loved one or friend died from it. Furthermore, the Coronavirus Act has effectively placed them under house arrest.
In other words, if the MCCD signing doctor hasn't seen the patient, while they were alive, no further inquiry is necessary. The qualified informant can be someone who has neither met the deceased nor knows anything about the circumstances surrounding their death.
In this situation, but only for COVID 19 deaths, it is fine to assume the death was from the disease. If you, the coroner, don't like the idea, don't make a fuss. Just sign the damn thing or else.
Impacting The COVID 19 Statistics
This quite bizarre death registration process compelled the ONS to issue guidance to doctors signing MCCD's. Not only is there no need for an examination to pronounce death from COVID 19, nor is there any necessity for a positive test or even an indicative CT scan.
In their guidance the ONS advised doctors on what constitutes an acceptable underlying cause of death. When mortality statistics are used for research it is usually the most relevant factor. The vast majority of COVID 19 deaths reported by the State and the MSM also reflect its identification as the underlying cause.
The World Health Organisation (WHO) define this as:
"The disease or injury which initiated the train of morbid events leading directly to death."
For COVID 19, this determination can be based upon the clinical judgement of a doctor who has never met the deceased. Quite possibly following nothing more than a video link consultation or a case note review of symptoms.
The problem is the symptoms of COVID 19 are largely indistinguishable from a range of other respiratory illnesses. A study from the University of Toronto found:
"The symptoms can vary, with some patients remaining asymptomatic, while others present with fever, cough, fatigue, and a host of other symptoms. The symptoms may be similar to patients with influenza or the common cold."
Nor is there any requirement for a post mortem to confirm the presence of COVID 19. Guidance from the Royal College of Pathologists states:
"If a death is believed to be due to confirmed COVID-19 infection, there is unlikely to be any need for a post-mortem examination to be conducted and the Medical Certificate of Cause of Death should be issued."
Clear causation between the underlying cause and the direct cause is imperative to establish the fact. Just because someone tested positive for the SARS-CoV-2 (SC2) virus it doesn't mean they developed the associated syndrome of COVID 19.
The Oxford Centre for Evidence Based Medicine found that anything between 5% - 80% of people who tested positive for SC2 did not have any symptoms of COVID 19. Asymptomatic people do not have a disease which impacts their health in the short term. Even for those who did test positive for SC2, claims that this was the underlying cause of death are dubious in an unknown number of cases.
Following the Coronavirus Act, in keeping with advice from the NHS, the ONS advised doctors:
"If before death the patient had symptoms typical of COVID 19 infection, but the test result has not been received, it would be satisfactory to give ‘COVID-19’ as the cause of death....In the circumstances of there being no swab, it is satisfactory to apply clinical judgement."

This isn't unique to COVID 19. Doctors are required to complete MCCD's "to the best of their knowledge and belief" even when test results may not yet be available. The difference in the case of COVID 19 is that all the normal requirements for qualified confirmatory opinions and every opportunity to question the cause of death have been removed.
In addition, the need to complete Cremation form 5, requiring a second medical opinion, has been suspended for all COVID 19 deaths. Given that post mortem confirmation is also extremely unlikely and agreement from a coroner is all but assured, this means possible COVID 19 decedents can be cremated without any clear evidence they ever had the disease.
In light of all the other registration oddities for determining COVID 19 mortality, the direct causation, proving COVID 19 was the underlying cause of death, appears extremely doubtful. We just don't know how many people have died from COVID 19. We are told many people have, but we cannot state with any certainty what the numbers are. Neither can the ONS.
Obviously concerned about the implications, the Royal College of Pathologists (RCPath) have called for a systemic post outbreak review. The Health Service Journal reports that the RCPath expects a detailed investigation into causes of death due to the degree of uncertainty.
Statistically It Get's Worse
The overwhelming majority of medical and care staff, coroners, pathologists, ONS statisticians and funeral directors have no desire to mislead anyone. However, in the case of COVID 19 deaths, the State has created a registration system so ambiguous it is virtually useless. The statistical product recorded by the ONS, despite their best efforts, is correspondingly vacuous.
This hasn't stopped the State and the MSM from reporting every death as proof of the deadliness of COVID 19. Claims of COVID 19 as the underlying cause of death should be treated with considerable scepticism.
Initially the daily reports were based upon the figures of COVID 19 deaths released by the NHS via the DHSC. These were the numbers with positive test results. The ONS also recorded positive test registrations from the NHS, care settings and the community.
As discussed, a positive test for SC2 doesn't necessarily mean you suffered any health impact from COVID 19. In addition, the test itself has proved to have a varying degree of reliability.
Nonetheless, the ONS figures from all settings, were higher than those reported by the MSM and the State in their daily briefings. However, the reliance upon positive tests changed on March 29th.

The State instructed the ONS not only to record all registered COVID 19 deaths, where positive tests results were known, but also where COVID 19 was merely suspected. In combination with the possibly spurious attribution from hospitals, this 'mention' of COVID 19, further distanced the statistics from clear, confirmed causes of death.
This prompted a significant increase in the COVID 19 fatalities reported by the ONS. Not because more people were dying from it, but because the categorisation of COVID 19 deaths had changed. Any mention of COVID 19 anywhere on the death certificate, regardless of other comorbidities, such as heart failure or cancer, were now recorded as registered COVID 19 deaths by the ONS.
This addition of claimed COVID 19 deaths has punctuated the ONS data throughout the outbreak. While we are told by the MSM that these new figures better reflect the reality of COVID 19 mortality, in truth we are moving further away from any meaningful record.
The evidence suggests the methodology has been altered at opportune moments to inflate and maintain the mortality statistics. Just after the virus peak of infection and the start of the lockdown, the State instructed the ONS to include suspected "mentions" of COVID 19. Again, as the recorded numbers of deaths were dropping, the State started releasing more figures from the care sector. From April 29th they have introduced additional figures provided by the Care Quality Commission (CQC).
If the figures from the NHS are at best questionable, the figures from the CQC run the risk of moving us into fantasy land. All the same problems of decedents not being seen, video consultations, lack of corroborative medical opinion and so forth remain. However, in care settings the onus for signing MCCD's shifts from hospital doctors to General Practitioners (GP's).
The CQC is the independent regulator of health and social care in England. During the COVID 19 outbreak it has not required care homes or community care providers to notify them of suspected cases. It has also suspended all inspections.
From the 29th April the CQC will provide statistics to the ONS where a "care home provider has stated COVID-19 as a suspected or confirmed cause of death." This notification is made online via the CQC's Provider Portal. Provisional figures will be included in the ONS daily updates.
The CQC is tasked with making sure decedents from care homes who died in hospital are removed from the reports before submitting them to the ONS. Otherwise massive duplication will occur. We can only hope statisticians will be extremely diligent.
The ONS has reported what these statistics from the CQC will be based upon. Frankly, it makes jaw dropping reading. The ONS state:
"The inclusion of a death in the published figures as being the result of COVID-19 is based on the statement of the care home provider, which may or may not correspond to a medical diagnosis or test result, or be reflected in the death certification."
Most care home providers are not medically trained. Their judgement regarding whether or not the decedent had COVID 19 may well be the result of a once weekly phone call with a GP. Guidance to GP's from NHS England states that Possible COVID 19 patients should be identified primarily by weekly check-ins online.
This is in keeping with the NHS Key Principles of General Practice, in relation to COVID 19, which states:
"Remote consultations should be used when possible. Consider the use of video consultations when appropriate."
The ONS add:
"There is no validation built into the quality of data on collection. Fields may be left blank or may contain information that is contradictory, and this may not be resolved at the point of publication. Most pertinent to this release are place of death and whether the death was as a result of confirmed or suspected coronavirus."
This is the system the CQC will use to collect the data for the ONS reports. Once someone, either in a care home or cared for in the community, is assumed to have died of COVID 19, based upon the best guess of the care provider following a chat with a local GP, in keeping with the process we have already discussed, their MCCD will be signed off as a COVID 19 death. The ONS will add their death to the COVID 19 statistics and the State and the MSM will report them to the public as confirmed COVID 19 mortality.
How anyone can consider the statistics from care providers an accurate and reliable record of COVID 19 deaths is difficult to envisage. Nonetheless, that is what we are asked to believe.
The State And MSM COVID 19 Fudge
All we are able to identify with any certainty are the total number of of all deaths, called all cause mortality, reported by the ONS. We cannot be confident about what caused those deaths during the COVID 19 outbreak.
The State has presided over a truly remarkable bastardisation of the ONS data for COVID 19. This has not only rendered records of COVID 19 deaths a statistical black hole but, during the claimed pandemic, has also made the ONS data for other causes of excess mortality practically unknowable.
Especially for the ONS, any chance of accurately separating COVID 19 deaths from other causes of mortality has been completely obliterated by State diktat. For the first time in their history the ONS are reporting a relatively large number of highly dubious registered causes of death. However, they remain our best hope of knowing how many people have passed away.
In the meantime, while we wait for the ONS data to emerge, the MSM are reporting every COVID 19 death from any source they can find. Some are vaguely confirmed and some not. They are also reporting suspected COVID 19 deaths from care homes, provisional figures from the NHS , the CQC and then the same figures again from the DHSC and later the ONS.
The narrative they are presenting, on the back of this hodgepodge of statistical irrelevance, is designed to convince the public of the severity of the outbreak in the UK. There is clearly high excess mortality at the moment. Thanks to the lockdown, this is happening while the NHS is essentially closed to everyone other than suspected COVID 19 patients.

Early studies have already predicted a significant health impact from the lack of essential health care caused by the lockdown. People requiring treatment for a range of other potentially fatal conditions aren't getting it. This was acknowledged by the UK's Chief Medical Officer Chris Witty in the daily briefing on April 30th:
"...You have the direct deaths from coronavirus but also indirect deaths. Part of which is caused by the NHS and public health services not being able to do what they normally can to look after people with other conditions....It is therefore important.....to do the other important things like urgent cancer care, elective surgery and all the other thing like screening....which we need to do to keep people healthy."
How many people have died of other causes, due to the lockdown, only to be registered as COVID 19 deaths? We just don't know and the ONS have no way of finding out.
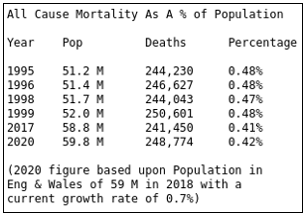
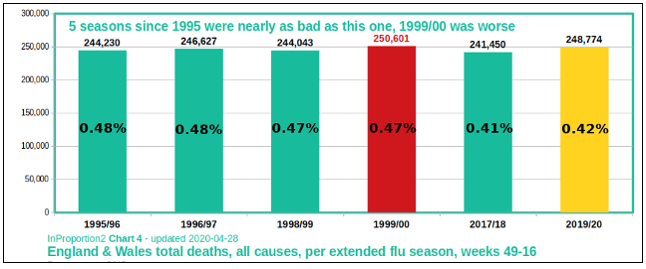
However we do know, thanks to the ONS, the total all cause mortality as a percentage of population in England and Wales over recent decades. This analysis shows us, while excess mortality this year is high, it is by no means unprecedented. In fact, as a percentage of population, it is notably lower to the comparable years of 1995, 1996, 1998 and 1999. Yet none of these years necessitated the shut down of the economy nor the dire health consequences of closing the NHS to all but a few patients.
Between 27th March and 17th April (ONS weeks 14,15 & 16) the ONS registered 25,932 additional deaths above the statistical recent 5 year norm. Of these 11,427 recorded COVID 19 as the sole mentioned underlying cause.
We have just explored the considerable doubt about this attribution. However, if we accept this figure, it means the remaining 14,505 people died with other registered underlying causes. That means approximately 56% of additional excess mortality is attributable to something else, either in addition to or entirely separate from suggested COVID 19.
Given this inexplicable Spring mortality it seems highly likely these are at least some of the indirect deaths the UK's Chief Medical Officer spoke of. To claim all these excess deaths are the result of COVID 19, as the State and MSM persistently do, is without any justification whatsoever.
It is not possible to identify how many people have died as a direct result of COVID 19 either from the registration of deaths or the resultant statistics. This is not the fault of medical practitioners or statisticians. It is caused by a State response to a claimed pandemic which has rendered the most crucial processes, and the data gleaned from them, a statistical nonsense.
Take it easy you hoopy froods.
