In 2022, a 45-year-old woman with no known underlying diseases was referred due to sudden oppressive chest pain lasting for 3 hours associated with nausea and dyspnea at rest. Physical examination with a normal state of consciousness, heart rate 71bpm, blood pressure of 110/50 mmHg, cardiopulmonary auscultation revealed an S3 gallop and bibasilar rales. There was no jugular vein engorgement, and the other findings were unremarkable.
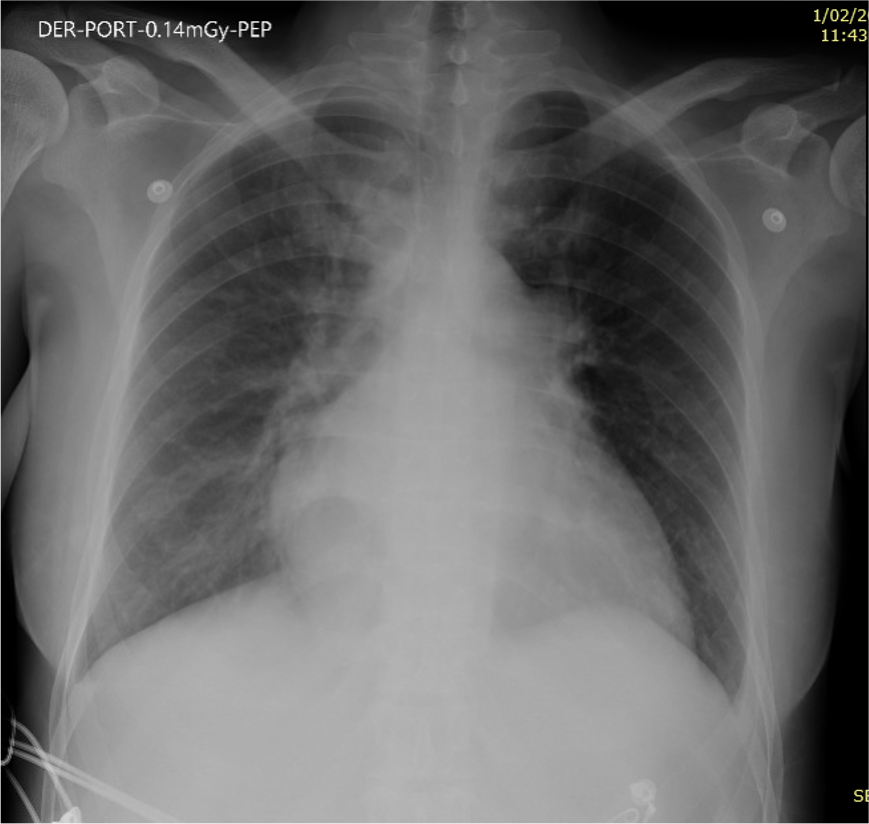
A chest X-ray was performed showing enlargement of the cardiac silhouette and bilateral interstitial infiltrates consistent with stage 2 acute pulmonary edema (Fig. 1).
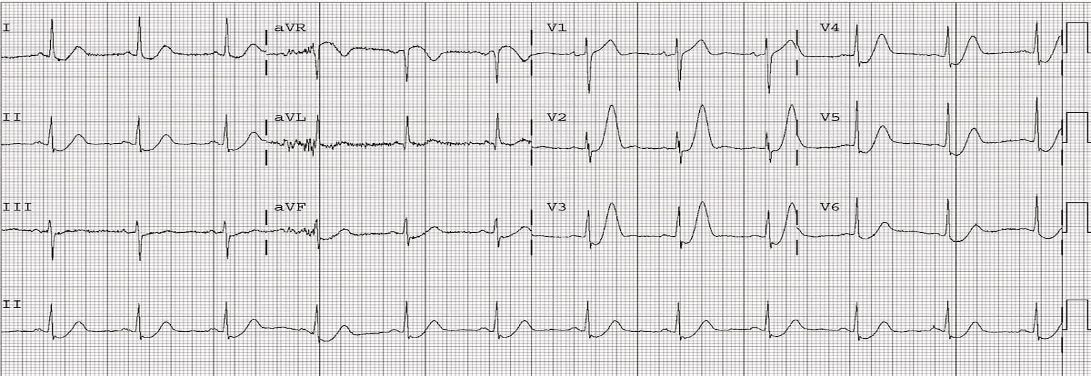
The electrocardiogram (ECG) revealed upsloping ST segment depression with prominent and symmetrical T waves in the precordial leads and reciprocal ST segment elevation in aVR compatible with winter ECG pattern (Fig. 2).
Hemogram, plasma creatinine, urea and electrolytes tests were normal and troponin I was 0.15 ng/ml [Normal value (NV): less than 0.06 ng/ml].
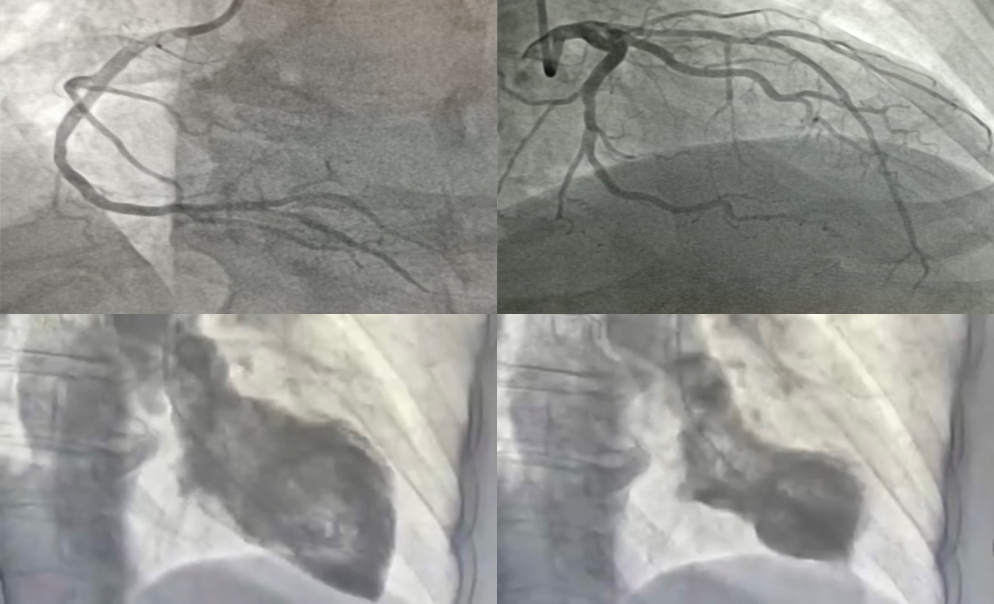
Coronary angiography was done due to the initial suspicion of acute coronary syndrome (ACS) and the results showed that the coronary tree was free of lesionsand ventriculography revealed significant ventricular dysfunction, with hypercontractility of the most basal segments and akinesia of distal ones, consistent with Takotsubo syndrome (Fig 3).
These findings were also found in the Doppler echocardiogram.
The patient was interrogated again and mentioned symptoms such as tremors, agitation, palpitations, and diarrhea throughout the previous three weeks. Thyroid function test revealed a free thyroxine 4 (FT4) value of 82.3 pmol/L (NV: 10-28.2), thyroid stimulating hormone (TSH) <0.01 mIU/L (NV 0.45-4.16), TSH receptor antibody (TRAb) 9.2 IU/L (NV<3.5) and the thyroid echography showed moderate enlargement of the thyroid gland, without nodules; being consistent with Graves' disease diagnosis.
The Burch-Wartofsky point scale (BWPS) indicated an imminent thyroid storm; therefore, antithyroid medication (Methimazole 10 mg every 8 hours) and beta blockers (Propranolol 40 mg every 6 hours) were initiated with positive clinical and analytical progress (Table 1).
A cardiac magnetic resonance (CMR) was performed on the patient six days after admission, and the results showed that the left ventricular function and contractility abnormality had returned to normal.
The patient was discharged with outpatient follow-up by cardiology and endocrinology teams.
Congratulations @cklm1993! You received a personal badge!
You can view your badges on your board and compare yourself to others in the Ranking
Check out our last posts:
Support the HiveBuzz project. Vote for our proposal!