
A few days ago I attended a workshop on HIV/AIDS in Muscat and I came to know some new information on it. In a series of posts, I am going to share that information.
Like DM or hypertension, PLHIV (people living with HIV/AIDS) can lead a normal life. And they have to take ART (Anti-Retroviral Therapy) lifelong just like anti-diabetic and anti-hypertensive medicines.
In my previous post, I talked about the global HIV/AIDS status. Today, we will know about the transmission of HIV from one person to another.
Before learning the various ways of transmission, we need to shed light on a few things. Besides blood, the viruses are found in a wide range of body fluids and tissues but the majority of infections are transmitted via seminal fluid, vaginal or cervical fluids (and definitely blood). The risk of contracting HIV after exposure to infected body fluid depends on the integrity of the exposed site, the type & volume of the fluid, duration of exposure to the infected fluids and level of viremia in the source person. That means following a single exposure, it won’t confirm that you will definitely get the HIV. On the other hand, you have every chance of contracting HIV if the above-mentioned criteria are found in favour of HIV transmission (such as ulceration in the exposed site, high level of viremia in the infected fluids etc.)
HIV does not infect all the cells in our body or immune systems. They have some specific targets. HIV only infects the cells which are bearing the CD4 receptor (CD4+ cells). In our last post, we have seen that T-helper lymphocytes (most important), monocyte-macrophages and dendritic cells are the cells which carry CD4 receptors on their cell membrane. That means HIV infects these cells only.
HIV is primarily transmitted by
- Sexual contact (both heterosexual and male to male)
- Blood and blood products, and
- Infected mother to the infants (during pregnancy, during delivery or via breast milk)
- There is no evidence of HIV transmission by (a) Casual contacts & (b) Insects such as a mosquito bite
Here is the estimated per-act probability (by exposure act) of acquiring HIV from an infected source (Risk per 10,000 exposures)
![]()
From the above table, we can see that transfusion of blood from a patient having HIV is the main method for transmission of the virus. Following a single transfusion of such blood or blood products, the recipient has a 92.5% chance of contracting the virus. The third most common method is homosexuality between male to male. The passive partner (Receptive anal intercourse) has the 1.38% chance of having the HIV from his partner following a single enjoyment (!) provided that the active one is HIV positive. On the other hand, the donor (Insertive anal intercourse) partner (!) has only 0.11% chance of having the virus if the passive partner is an HIV carrier. The chances of transmission during oral sex are very low.
![]()
HIV among various population groups
In the last post we can see that, globally, more female is living with HIV than male. In a heterosexual relationship, a female has 0.08% chance of having HIV from a single sexual penetration from an HIV positive husband or partner. Vice versa, the male partner’s chance of getting HIV is 0.04%.

Men Vs Women suffering from HIV/AIDS
Another major method of transmission of the virus is from HIV infected mother to her child, and during vaginal delivery, the newborn has a 15% chance of getting the virus from his/her mother. But two studies which were conducted in Rwanda and the Democratic Republic of Congo showed that the relative proportion of mother to child transmission of HIV were 23-30% before birth, 50-65% during birth and 12-20% via breastfeeding. Various virologic analyses of the aborted fetuses indicated that HIV can be transmitted from mother to the fetus during the 1st and 2nd trimester of pregnancy.
As now we know all the methods of transmission of the HIV, lets us get some answers on HIV.
Why a male partner with genital infection does more transmission of HIV than non-genital infectious male?
HIV is demonstrated in seminal fluid either within mononuclear cells (CD4 positive cells) or in cell-free materials. It is seen that the concentration of the virus in seminal fluid is more if the number of lymphocytes and monocytes are also more in the fluid because these are the target cells of the HIV. We already know that these cells are part of the immune system of our body and go into the battlefield to fight with invading microorganisms. Considering this, if the male part is having any kind of inflammatory conditions in his genital organs, (Not STIs; simple infections) e.g. urethritis, prostatitis or epididymitis, the mononuclear cells will be found abundantly in his seminal fluids. As a result, the virus will be more in seminal fluid.
Why does the female get more infection than the male during unprotected sexual intercourse?
According to the latest HIV/AIDS data (2017), globally, 18.2 million women are living with HIV while for men it is 16.8 million. From the above table we can also see that following an unprotected sexual intercourse, the chance of getting the HIV for male and female is 0.04% and 0.08% respectively, provided that one part is having the virus. Why is this difference? It is mostly due to two factors:
- Prolonged exposure to the infected seminal fluid to the vaginal, cervical mucosa and the endometrium (following deposition of seminal fluid in the female genital tract)
- Brief exposure of the penis and urethral orifice to the infected vaginal fluid
The same explanation is applicable to the increased transmission in receptive anal intercourse (passive partner).
Why does anal intercourse transmit more viruses in comparison with penile-vaginal intercourse?
From the table and above discussion, it is clear that following unprotected receptive anal intercourse (URAI), the chance of contracting the virus is more than receptive vaginal intercourse. Why is that? One of the factors is the difference between the layer of the vaginal mucosa and that of the rectum and anal canal. A thin layer of the mucous membrane is separating the infected seminal fluid from the underlying blood vessels and susceptible cells which is very fragile and prone to microtrauma. On the other hand, the vaginal mucosa is several layers thick and less likely to be traumatized during intercourse.
Another factor is the nature of sexual practice. If anal douching is used or any other form of sexual practice is done (other than penile penetration) that traumatize the rectal mucosa also increase the likelihood of infection. Even without the microtrauma, due to the presence of abundant susceptible cells (e.g. Langerhans cells) just beneath the very thin mucosa, the infection may happen.
In a nutshell, the anal intercourse provides at least 2 modalities of HIV infection:
- Direct inoculation of the virus into the blood in case of traumatic tears in the mucosa
- In the absence of trauma, infection of the susceptible target cells, such as Langerhans cells.
Why the presence of other STIs (sexually transmitted infections) increases the chance of transmission of HIV following unprotected sex?
Usually, there are two types of STIs; Ulcerating and non-ulcerating STIs. Treponema pallidum (causes syphilis), Haemophilus ducreyi, and herpes simplex virus are important causes of genital ulcerations linked to the transmission of HIV. On the other hand, Chlamydia trachomatis, Neisseria gonorrhoeae, and Trichomonas vaginalis are non-ulcerative inflammatory STIs which are also associated with transmission of the virus. Bacterial vaginosis, which is not strictly an STI, also may be responsible for an increased risk of transmission of HIV infection.
Regarding ulcerating STIs, we know the explanation. As the mucous member is not intact, the HIV can easily get entry into the blood and attack the susceptible target cells. But how the non-ulcerating STIs are responsible? It is seen that due to the infections, the inflammatory cells which are happened to be susceptible targets of the virus, are found abundantly within the mucosa and underlying tissues of the genital tract. If other criteria of infectivity are fulfilled such as high viral load, prolonged exposure etc. then the virus may transmit into a person.
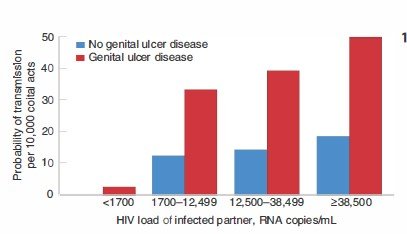
From the above chart, we can see the effects of the presence of genital ulcer diseases on the transmission of HIV. For example, with a load of 15,000-38,499 copies/mL, if no genital ulcers, the chance of getting the HIV after a single coital act is less than 0.20%. But in the presence of genital ulceration, the chance is around 0.4%; almost 2-3 times higher!
Does treating STIs reduce the chance of infection?
Yes. Several studies depict that treating STIs and genital tract syndromes may help to prevent the transmission of HIV except for HSV (herpes simplex virus). Despite anti-HSV therapy which results in healing of HSV related genital ulcers; the transmission of HIV is not reduced. It was revealed by biopsy studies that unlike other SITs, HIV receptor positive inflammatory cells (CD4+ cells) persisted in the genital tissue despite the healing of the ulcers. In other words, HIV susceptible target cells remained at the site.
Does circumcision prevent HIV transmission?
Yes. Circumcision does prevent the HIV transmission. A number of studies have proven that circumcision is associated with a lower risk of getting the HIV for a heterosexual male. In case of homosexual men, data suggest that circumcision is protective in those men who are Insertive only. It poses the question “why uncircumcised men are susceptible to HIV? Here are the possible reasons:
- Uncircumcised men are more prone to have STIs.
- Microtrauma to the foreskin (as well as glans penis)
- The highly vascular inner foreskin contains a high density of HIV targets cells such as Langerhans cells, CD4+ T helper cells, macrophages etc.
- The moist environment under the foreskin favours the colonization and persistence of microbial flora which in turn bring inflammatory changes locally.
Does OCP as a contraceptive method has an effect on HIV transmission?
Unfortunately, yes! In some studies, it is shown that the incidence of transmission is higher among the OCP using-women in comparison with the non-users. The likely explanation is the drug-induced changes in the female genital tracts e.g. cervical mucosa which renders it more vulnerable to penetration by the virus.
Adolescent girls may be more susceptible to the virus upon exposure because of immature genital tracts with increased cervical ectopy or exposed columnar epithelium.
Can anyone get HIV following oral sex?
The chance is extremely low. However, there are well-documented reports of transmission of HIV from perverted sexual activities such as fellatio (oral stimulation of man’s penis) or cunnilingus (an Oral sexual act performed by a person on female genitalia- Wikipedia). As a result, “Oral sex is completely safe”, this statement is no longer valid.
Do alcohol consumption, illicit drugs and sex stimulants have effects on HIV transmission?
They don’t have any direct effects but these lead to risky sexual behaviour, especially among men who have sex with men, resulting in doing “unsafe-sex”. Alcohol consumption, methamphetamine and other so-called club drugs (For example ecstasy, ketamine, gamma-hydroxybutyrate etc.), and PDE-5 inhibitors (for example sildenafil is widely known as Viagra, tadalafil, vardenafil etc.) have been associated with extreme and risky sexual behaviours.
I was an injection drug user and may have shared needles once or twice before. Am I having the HIV?
The chance of contracting the virus from a single act of needle sharing in perspective of injection drug use (IDU) is around 0.63% only. But in certain conditions, the chances may go higher, such as:
- The duration of injection drug use
- The frequency of needle sharing
- The number of partners whom with the needles were shared
- Presence of other psychiatric conditions such as antisocial personality disorder
- The use of cocaine in injectable form or smoked as "crack", and
- The use of injection drugs in a geographic location with a high prevalence of HIV/AIDS
Look at the lists and find out your mistakes.
Is our whole body contaminated with the HIV or only few body fluids?
Already we have mentioned that blood, seminal fluid and vaginal fluids are considered as the main contaminated fluid through which one can contract the virus from others. But in a more accurate sense, any kind of body fluids may contain the virus and risks of transmission via them are present. Here is the list:
- CSF (cerebrospinal fluid): Found within the brain and spinal cord
- Synovial fluids: Found in our joint spaces
- Pleural fluid: Around the lungs
- Pericardial fluid: Within the sac which contains the heart
- Amniotic fluids: Within which the fetus floats
- Visible blood on faeces, nasal secretion, saliva, sputum, sweats, tears, urine, and vomitus
These are particularly important for health-related personals. Needlestick injury contaminated with above-mentioned fluids, along with the blood, of course, may pose the risk of contracting the virus.
My wife became pregnant recently and we both are HIV positive. Will our baby surely have it too?
If she is on effective ART (anti-retroviral therapy) and viral load is undetectable, the chance is extremely unlikely. The maternal viral load is one of the main factors to determine the risk of vertical transmission. The transmission is very unlikely if the level of mother’s plasma viremia is < 1000 copies of HIV RNA/mL. If the level is below 50 copies/mL which, by definition, it is called “undetectable”, the chance is extremely unlikely. You should also keep in mind that during vaginal delivery the transmission from mother to the baby is the highest. The time difference between the rupture of the membrane and the final delivery is very crucial. The longer the duration, the higher the chance of transmission.
Written By @Hafiz34
References:
- Harrison’s Principles of Internal Medicine 2 volumes 19th Edition; 1220
- Davidsons Principles and Practice of Medicine 23 edition; 308
Posted from myAirClinic Healthcare App. Download Android Version from PLAYSTORE!
Wow! That's quite informative! I remember growing up they made it sound like vaginal intercourse would almost certainly transit the disease. But it's less than 0.1% chance either way? That makes it sound less scary definitely.